By: Dr. Rahat Aisha Yasmeen, Freelance Health Writer and Datelinehealth Africa (DLHA) volunteer, with Editorial staff support.
Cleft-lip and palate is a non-communicable, disfiguring abnormality of the lower lip and neighboring parts of the mouth that occur in a developing baby during pregnancy and is present from birth (i.e. congenital).
It is a disorder that is associated with poverty and is commoner in lower and middle income countries.
Its prevalence differs by gender and ethnicity. Boys are more affected than girls with a reported ratio of 2:1 for cleft lip and/or cleft lip and palate, whilst females have a slightly greater risk for cleft palate only.
In South Africa, cleft lip and palate are underreported and remain in the top five of most common congenital disorders.
Clefts are formed during pregnancy when tissues fail to come together to properly form the lip (usually upper lip), bones of the root of the teeth (usually the upper jaw; i.e. alveolus) or palate. This disruption of migration of tissues in turn causes a variety of non-fusion abnormalities between lips and palate, extending towards nose, mouth or eyes as shown in figure 1.
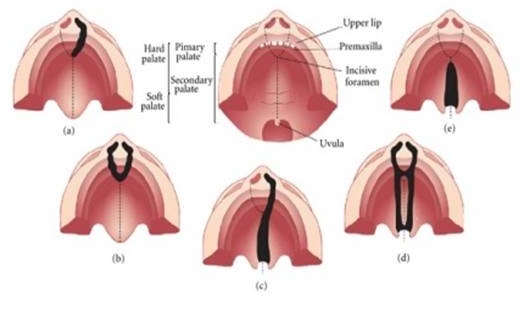
Figure 1. Representation of the most common types of cleft affecting the palate. (a) Unilateral cleft lip with alveolar involvement; (b) Bilateral cleft lip with alveolar involvement; (c) Unilateral cleft lip associated with cleft palate; (d) Bilateral cleft lip and palate; (e) Cleft palate only.
Click on image to enlarge. Credit
Clefts have complex cause involving:
Genetic causes may be due to:
Environment risk factors include:
Clefts are common birth defects. In fact, globally, 1 in every 700 babies is born with a cleft lip and/or palate.
The prevalence in African populations generally is usually derived from hospital-based data and is known to be lower at 1 in every 2,500 babies.
The prevalence in South Africa has been estimated at 0.3 per 1000 live births, with provincial variation of 0.1/1000 to 1.2/1000. For comparison, the highest incidence globally is in Asia and South Americas at an average of 2 per 1000 live births. The incidence in China is reported to be 1.663 per 1000 live births.
The burden in a sample of other African countries ranges as shown in Table 1.
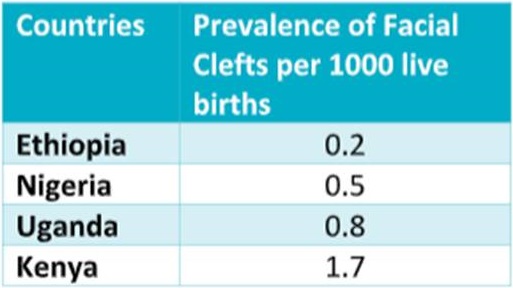
Table 1: Shows the burden of Orofacial clefts in a sample of African countries. Click on image to enlarge. Source.
Compounding this shortage of trained personnel is the huge need for oral care in the region. As at 2019, 480 million Africans were estimated to have oral diseases and in need of care. 60% of children suffering from oral diseases get no care at any given time.
It is clear from this unwholesome situation that children with cleft lip and palate will lack the specialized care that is needed to repair their disfigurement.
The South Africa Medical Research Council’s Environmental and Health Research Unit conducted a study on 2515 cases of children born with cleft conditions countrywide. The study showed that mothers of these children lived during pregnancy in various ‘hotspot’ areas with higher concentrations of smoke and dust particles in the air. Fewer cases of cleft conditions were seen in areas with lower levels of air pollution. The study was reported by Operation Smile, South Africa,
The findings of the study led the Chief Specialist Scientist of the research institution, Dr. Caradee Wright; to believe that enough evidence existed to show that environmental pollution probably impacts the development of cleft conditions. Air pollution levels are known to be high in South Africa. Domestic fuel burning, coal-fired power stations, traffic, mining and industry all contribute to the problem.
According to the WHO Africa, the diagnosis and treatment of clefts continue to present a significant challenge to public health, particularly in lower-middle income countries like South Africa where availability, access to and affordability of complex multidisciplinary care are limited and complications from untreated clefts result in high rates of infant mortality.
What more can be done to lower the burden of clefts in South Africa?
Efforts to lower the burden of cleft lip and palate in South Africa, calls for action in many ways as follows:
1. Intensive monitoring and evaluation of existing oral health intervention programs is needed to understand their effectiveness and improve on what works while discontinuing what doesn’t.
2. The South African government should improve on existing policies and programs as well as institute new ones as needed, for clean air promotion and reduction in environmental pollution as well as reduction in the numerous inequities common in low-middle income communities in the country.
These inequities, such as in housing, access to education and affordable care, healthy nutrition and income distribution, etc., are driven by complex socio-economic, educational and structural systems that directly and indirectly impact the occurrence of clefts in the country.
3. The Ministry of Health should support more research that will inform policy and programmatic decisions to facilitate evidence-based delivery of multi-disciplinary oral health services at the level of provincial health departments.
4. All concerned governmental and non-governmental stakeholders, including communty leaders and members should collaborate and engage in continuous awareness raising and education in at risk communities about the causes, risk factors and care of clefts so as to improve early presentation to caregivers. Such efforts will serve to decrease the number of cases and more importantly, decrease the rate of permanent oral deformity in the South African population.
In 15 years of operation, charitable entities like the Smile Train organization have enabled repair of over 1,000,000 clefts in 87 countries, and many of these repairs have been in the African continent (see figure 2).

Figure 2: A successful case carried out by Smile Train organization to repair cleft lip. Click on image to enalrge. Credit.
Despite organizations such as Operation Smile South Africa, Smile Train, Smile Foundation and Cleft Friends amplifying their efforts to reach out to cleft patients, a significant impact of these broad outreach on the burden of cleft in Africa remains to been seen.
More evidence-based preventive and coproduction public health interventions are needed in addition to the surgical repair programs of the charity organizations.
Carrim F, Hlongwa P. Profile of cleft lip and palate patients at a dental hospital in Johannesburg, South Africa. J Cleft Lip Palate Craniofac Anomal 2022;9:139-44.
Operation Smile South Africa. Link between air pollution and cleft conditions. March 6 2023. Accessed May 13, 2023.
Bhayat A, Chikte U. Human Resources for Oral Health Care in South Africa: A 2018 Update. Int J Environ Res Public Health. 2019 May 14;16(10):1668. doi: 10.3390/ijerph16101668. PMID: 31091648; PMCID: PMC6571692.
Gallagher JE, Mattos Savage GC, Crummey SC, Sabbah W, Varenne B, Makino Y. Oral Health Workforce in Africa: A Scarce Resource. Int. J. Environ. Res. Public Health 2023, 20, 2328. https:// doi.org/10.3390/ijerph20032328.
Hlongwa P, Levin J, Rispel LC. Epidemiology and clinical profile of individuals with cleft lip and palate utilising specialised academic treatment centres in South Africa. PLoS One. 2019 May 9;14(5):e0215931. doi: 10.1371/journal.pone.0215931. PMID: 31071123; PMCID: PMC6508722.
Hlongwa P, Rispel LC. Coproduction in the management of individuals with cleft lip and palate in South Africa: the Ekhaya Lethu model, International Journal for Quality in Health Care, Volume 33, Issue Supplement_2, November 2021, Pages ii33–ii39, https://doi.org/10.1093/intqhc/mzab082.
Conway JC, Taub PJ, Kling R, Oberoi K, Doucette J, Jabs EW. Ten-year experience of more than 35,000 orofacial clefts in Africa. BMC Pediatr. 2015 Feb 14;15:8. doi: 10.1186/s12887-015-0328-5. PMID: 25884320; PMCID: PMC4342189.
van Wyk PJ, van Wyk C. Oral health in South Africa. International Dental Journal, Volume 54, Supplement 6, 2004, Pages 373-377. https://doi.org/10.1111/j.1875-595X.2004.tb00014.x.
Zhu Y, Miao H, Zeng Q, Li B, Wang D, Yu X, Wu H, Chen Y, Guo P, Liu F. Prevalence of cleft lip and/or cleft palate in Guangdong province, China, 2015-2018: a spatio-temporal descriptive analysis. BMJ Open. 2021 Aug 2;11(8):e046430. doi: 10.1136/bmjopen-2020-046430.
Related:
Dental care in Africa: Challenges and solutions.
Published: May 23, 2023
© 2023. Datelinehealth Africa Inc. All rights reserved.
Permission is given to copy, use and share content without alteration or modification and subject to attribution as to source.
DATELINEHEALTH AFRICA INC., is a digital publisher for informational and educational purposes and does not offer personal medical care and advice. If you have a medical problem needing routine or emergency attention, call your doctor or local emergency services immediately, or visit the nearest emergency room or the nearest hospital. You should consult your professional healthcare provider before starting any nutrition, diet, exercise, fitness, medical or wellness program mentioned or referenced in the DatelinehealthAfrica website. Click here for more disclaimer notice.


