14 Breastfeeding Challenges African Nursing Mothers Need To Know
By: Chiamaka Wisdom-Asotah, MBBS, MPH. Freelance Health Writer and DLHA Volunteer. Reviewed by: Chika Jones, RN, RM, RPHN, BNSc.

An African Mother holding her baby in a cradle-hold position with an incandescent bulb glowing against a darkened background. Image credit: Freepik
Breastfeeding is the most important source of nutrition for your newborn. When it is the only source of food and fluids for your baby for the first six months of life, it is referred to as exclusive breastfeeding. However, breastfeeding can continue till your baby reaches two years of age during which additional sources of feeding can also be provided. [1, 2] Interestingly for many mothers, breastfeeding is not as easy as it seems, even though it’s a natural process.
Several breastfeeding challenges often hinder this new experience, and in fact, research shows that in Africa, the rate of exclusive breastfeeding is low. Despite these challenges, breastfeeding protects you from health conditions such as breast and ovarian cancers. Exclusively breastfed children are protected against infections and grow to have higher order brain function [3].
This article will explore the common breastfeeding challenges you may face as an African nursing mother and ways you can deal with them.
For ease of understanding, the common breastfeeding challenges will be discussed under those related to you the mother and those related to your baby (see fig. 1).
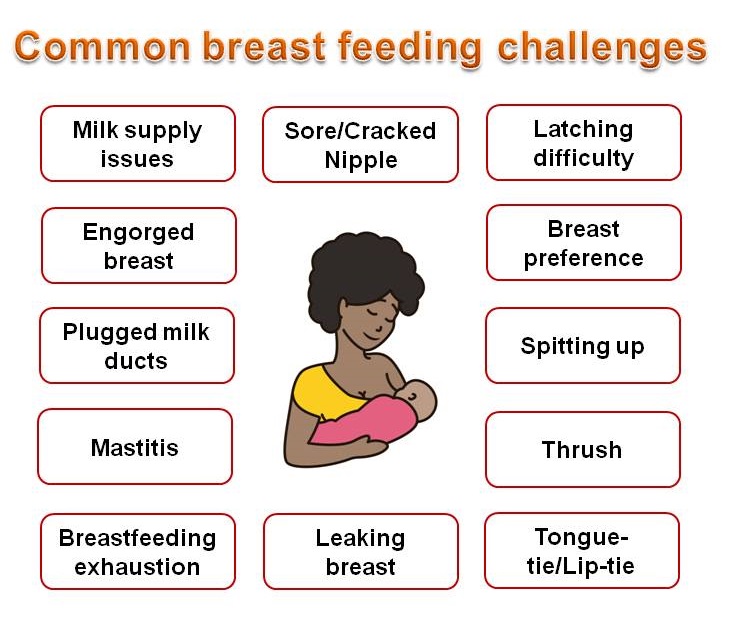
Fig. 1: Showing common breastfeeding challenges related to you, the mother or your baby. Click on the image to enlarge.
Cracked or sore nipples are very common, especially for new mothers [4]. They usually indicate that your baby is not attached correctly during feeds. You need to ensure your baby latches or attaches deeply and is well-positioned.
Other causes of nipple soreness include:
Let-down, also known as the milk ejection reflex, refers to the milk flow into your breasts. Oxytocin is the hormone responsible for this action. Usually, within 1-2 minutes of your baby’s fast suckling or breast pumping, a let-down should occur [5].
If these are present, then you need not worry.
a. Slow milk let-down
b. Fast/strong milk let-down
If your baby is bottle-fed, this may delay let-down, as your baby’s suckling pattern may not effectively stimulate your breasts. Women with medical conditions such as hypothyroidism, breast reduction and bleeding after delivery may also experience let-down problems. You need to consult your health practitioner for support in this regard.
Regarding a strong let-down, a few seconds after your baby starts suckling, they could choke a little. They may stop nursing and start crying because of the quick milk flow into their mouth.
To manage strong let-down:
Reduced milk supply is a common reason why most women wean their babies early, and research shows that it affects 10 to 15% of mothers. Human milk is easily digested, so your baby might feed frequently (8-12 times daily) [6].
Occasionally, mothers mistake this frequent feeding for insufficient milk volumes, but that’s not always the case.
Breastfeeding is a demand-and-supply process, meaning the more your baby feeds, the more milk you produce. However, no matter how much milk you produce, the quality remains the same and greatly benefits your baby [5].
Here’s what you can do
a) Steady weight gain
b) 6–8 wet diapers occur on average per day.
c) Stool colour changes from green to yellow by day five
If you’re not sure you’re producing enough, a healthcare professional should observe your breastfeeding process, give expert advice, and support you in feeding or expressing milk more frequently (8-12 times daily) to increase your supply [8].
Medications like galactagogues (i.e., breast milk producing drugs; e.g., domperidone) may be helpful for mothers who want to breastfeed their adopted babies but should not be used first before trying other solutions [6].
Within the first three to five days after delivery, most women experience breast engorgement. An engorged breast feels hard, swollen and lumpy. The pain can be uncomfortable for you, and your baby may have difficulties latching to take a suck.
Breast engorgement isn’t just caused by your breasts filling up. It happens when your breasts are not well emptied. As your baby learns to latch correctly, they suck enough to empty your breasts and prevent an engorgement. Engorgement can happen when your baby sleeps longer than usual, misses a feed or is being weaned off breastfeeding.
To manage engorgement, consider doing the following:
Some mothers wish for an oversupply with the intent of having their babies well-fed, but this doesn’t come without its challenges.
To treat an oversupply, try:
.jpg)
Fig. 2: Cartoon illustration of common breastfeeding positions. Click on the image to enlarge.
Plugged milk ducts (channels that transport milk from the breast to your baby’s mouth) are a common breastfeeding challenge. It means your milk channels are blocked. They can happen if feeds are skipped, your baby doesn’t feed well, or if you wear tight bras.
To treat a plugged milk duct, try the following:
Mastitis refers to pain, redness and swelling of the breast. It can be caused by an infection or breast engorgement. You may also have a fever if you have mastitis.
Mastitis occurs when there’s a blocked milk duct or build-up of milk. If mastitis is not treated promptly, it could cause a breast abscess (a painful build-up of pus in the breast). Breastfeeding is safe even if you have mastitis, and it helps to prevent engorgement that can worsen the condition [6].
Every new parent experiences exhaustion, especially in the first few weeks [5]. This is completely normal. Adjusting to your baby’s schedule will help you cope with this new phase. You might have to sleep when your baby is sleeping, even when you don’t feel like it, to enable you to rest enough.
To manage this, try:
As your breastfeeding gets established, you may start to notice your breasts leak at different times. You may experience leakage when your baby is nursing, when you think about them, hear them cry or go for long without nursing them. This is normal and shouldn’t get you worried. If you want to avoid this, then get your baby to feed as soon as you feel your breasts get full. Consider wearing nursing pads to help prevent milk stains, especially when you’re out and about.
1. Tongue Tie and Lip Tie
Tongue and lip tie conditions (see fig. 3) are common concerns for breastfeeding parents. Tongue-tie (also known medically as ankyloglossia), is a condition that occurs when the tongue is held down to the floor of the mouth in the midline by a tissue called frenulum. This may occur because the frenulum is too short, or tight thereby restricting tongue movements.
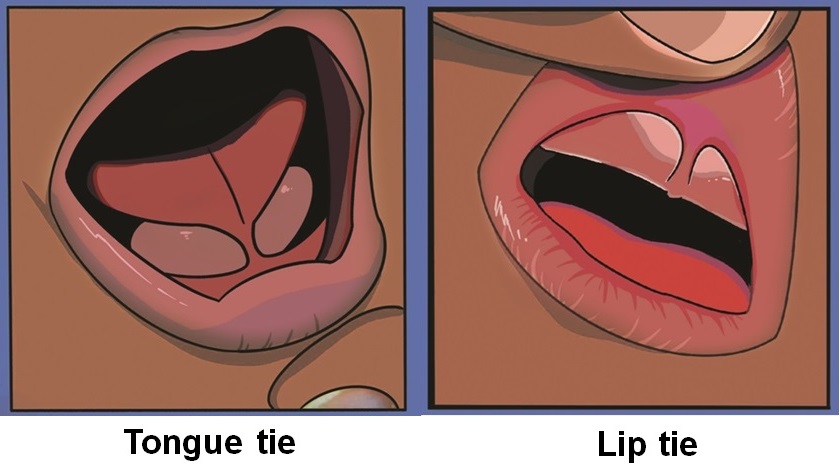
Fig 3: Cartoon illustration of tongue and lip ties in a baby. Click on imge to enlarge.
Lip tie on the other hand is less frequently seen compared to tongue tie. It is a condition that occurs when the frenulum connecting the upper or lower lips to the gums in the midline is too short, tight or thick thereby restricting lips movement.
This breastfeeding challenge can make nursing difficult because it limits your baby from moving their tongues and or lips easily.
Both conditions (tongue and lip ties) can affect breast and bottle feeding as well as speech development,
If you suspect your baby has a tongue or lip-tie, seek help from your baby’s healthcare provider.
While you wait for the help, try any of these:
Thrush is an infection caused by Candida albicans, a spore producing germ that feeds on moulds, yeast and mushrooms. The condition thrives in warm and moist areas and can affect the skin, nails, mouth and other parts of the body.
Oral thrush occurs when Candida albicans infection affects the mouth to form a flurry whitish coating on the tongue, gums and back of the throat (see fig 4).

Fig. 4: A balck child with oral thrush. Clickon image to enlarge. Image credit: Skin Deep
Having a cracked nipple makes you prone to having this infection and you can pass it on to your baby. If you or your baby has had antibiotics recently, then thrush could also happen.
To treat this, your provider will prescribe antifungal medications for use by you and your baby.
Babies spit up a lot and this is normal. In the first few days to weeks, they could take in more milk than they need and then spit out the excess [5].
If you’re concerned about this, try to address the following possible causes:
Consult your healthcare provider for further guidance if your baby spits up for hours or you feel concerned.
Some babies prefer one breast to the other. You may have noticed this with your little one. Though common, it often doesn’t last for long.
The reasons could be:
Encourage your little one to breastfeed from both sides so they can get enough milk. If this doesn’t work, allow them to feed on their preferred breast. You can express milk from the less preferred breast to maintain your supply and ensure your baby is full.
Your baby may have a challenge attaching to your breasts in the first few days of life. With time, they learn to do this effortlessly. If your baby doesn’t latch properly, breastfeeding can become challenging for both of you. You need to know how to achieve a good latch (see fig. 5) with your baby as they may refuse to nurse [5, 6], and if they do, you could end up with nipple injuries.
.jpg)
Fig. 5: Cartoon illustration of good and poor baby attachment (latching) during breastfeeding. Click on image to enarge.
You can contact the breastfeeding support team in your area to help you with this.
A: Bring your baby to your breasts and allow them to latch themselves. Also, make sure you’re using a position that suits you both [9]. If this doesn’t help, consult your breastfeeding specialist.
A: If your baby is gaining adequate weight, having 6-8 wet nappies daily and passing yellow stools, they’re probably getting enough milk.
A: It is rare to have a low milk supply because your body produces just what your baby needs per time. However, breastfeeding on demand and having a routine pumping schedule can improve milk production.
A: Unless indicated by your healthcare provider, trying to establish breastfeeding with your baby before introducing a bottle or pacifier is recommended. This can be around 3 – 4 weeks of age.
A: If you notice your baby isn’t gaining adequate weight, consult your healthcare provider so your baby can be thoroughly assessed and managed.
Breastfeeding challenges are common, and as a new mother, you could struggle to manage them properly. However, with proper knowledge and support, you can scale through and enjoy your breastfeeding journey.
1. World Health Organization. e-Library of evidence for nutrition action (eLENA). Exclusive breastfeeding for optimal growth, development and health of infants.[Internet] Last updated: 9 August 2023. [Cited March 30, 2025] Available from here.
2. US Centers for Disease Control and Prevention. Breastfeeding report card, [Internet]. February 24, 2025. [Cited March 30, 2025]. Available from here.
3. Kramer MS, Aboud F, Mironova E, et al. Breastfeeding and Child Cognitive Development: New Evidence From a Large Randomized Trial. Arch Gen Psychiatry. 2008;65(5):578–584. doi:10.1001/archpsyc.65.5.578. Available from here.
4. Babakazo P, Bosonkie M, Mafuta E, Mvuama N, Mapatano M-A (2022) Common breastfeeding problems experienced by lactating mothers during the first six months in Kinshasa. PLoS ONE 2022;17(10). Doi: 10.1371/journal.pone.0275477. Available from here
5. Bell A. Overcoming Common Breastfeeding Challenges. ]Internet]. UCLA Medical School, 28 July 2023. [Cited March 20, 2025]. Available from here.
6. The American College of Obstetrics and Gynecology. Committee opinion # 827. Breastfeeding Challenges. [Internet, n.d.]. Cited March 30, 2025. Available from here.
7. Jin X, Perrella SL, Lai CT, Taylor NL, Geddes DT. Causes of Low Milk Supply: The Roles of Estrogens, Progesterone, and Related External Factors. Adv Nutr. 2024 Jan;15(1):100129. doi: 10.1016/j.advnut.2023.10.002. Available from here
8. Kent, Jacqueline C., et al. ‘Principles for Maintaining or Increasing Breast Milk Production’. Journal of Obstetric, Gynecologic & Neonatal Nursing, vol. 41, no. 1, Jan. 2012, pp. 114–21.Available from here.
9/ OASH. Office of Women Health. DHSS, Getting a Good Latch. [Internet] Last updated Feb. 25, 2025. [Cited March 30, 2025]. Available from here.
Related:
Published: April 28, 2025
© 2025. Datelinehealth Africa Inc. All rights reserved.
Permission is given to copy, use and share content for non-commercial purposes without alteration or modification and subject to source attribution.
DATELINEHEALTH AFRICA INC., is a digital publisher for informational and educational purposes and does not offer personal medical care and advice. If you have a medical problem needing routine or emergency attention, call your doctor or local emergency services immediately, or visit the nearest emergency room or the nearest hospital. You should consult your professional healthcare provider before starting any nutrition, diet, exercise, fitness, medical or wellness program mentioned or referenced in the DatelinehealthAfrica website. Click here for more disclaimer notice.


