By Jennifer Orisakwe, DLHA Volunteer and Freelance Writer
In Nigeria, the uptake of contraception is low, with a 2021 UNICEF survey indicating that only four out of every ten women have their needs met for the use of any modern contraception. In the interest of good public health, contraceptive use by Nigerian women needs to improve considerably if they are to enjoy better sexual, reproductive, maternal and overall health outcomes during and after their child bearing life.
If you are African and live in Africa, there is a high chance that you might be able to point to a family that has more children than they can take care of.
The ability to plan and space pregnancies is a fundamental human right that has numerous benefits for women of reproductive age, their families, and society as a whole.
According to Ifeyinwa Akamike et al (2020), family planning uptake in Nigeria has remained low and this is as a result of the various challenges and barriers faced by women. Another 2020 study by Alo et al., quoted the most recent National Demographic and Household survey as reporting 17% and 37% contraceptive prevalence rates among married women and sexually active unmarried women between ages 15 to 49 years respectively with only 12% of the former using modern contraceptive methods and 28% of the latter doing so.
Such low level adoption of modern family planning methods in Nigeria, the most populous Sub-Saharan African, where population growth rates are high and maternal and child health indicators are poor, strongly confirms how highly essential family planning is to women in the reproductive age across Sub-Saharan Africa.
The Maternal Health Task Force (MHTF) at Harvard Chan School reports that family planning contributes up to 44 per cent reduction in maternal deaths, thereby making it key to safe motherhood,
By enabling women to control their reproductive health and make informed decisions about childbearing, family planning can improve maternal and child health, reduce poverty, empower women, and address population growth.
This article will explore the importance of family planning for Nigerian women of reproductive age and highlight the many benefits that can be achieved through its promotion and implementation.
According to the World Health Organization, family planning is defined as “the ability of individuals and couples to anticipate and attain their desired number of children and the spacing and timing of their births”. The process essentially allows people to attain their desired number of children, if any, and to determine the spacing of their pregnancies. It is achieved through the use of contraceptive methods.
Family planning is beneficial to Nigerian women of reproductive age for several reasons (Figure 1) including:
1. Improving maternal and child health: Family planning enables women to have children at intervals that are healthy for both the mother and the child. By spacing pregnancies, women are less likely to suffer from maternal complications such as hemorrhage, anemia, and prolonged labor. Additionally, children born to mothers who have practiced family planning are less likely to suffer from malnutrition, low birth weight, and infant mortality.
2. Addressing population growth: Nigeria has one of the highest population growth rates in the world, and family planning can help to slow this growth. Slowing population growth can have many benefits, including reducing pressure on resources, saving the environment and improving the overall quality of life for Nigerians.
3. Reducing poverty: Family planning can help to reduce poverty in Nigeria by enabling women to have fewer children and therefore be better able to provide for the children they do have. It can also reduce hunger and the strain on resources such as food, water, and healthcare.
4. Empowering women: Family planning can empower women by giving them greater control over their bodies and their lives. In so doing, it supports women’s ability to prosper in their sexual health and prevent the acquisition of sexually transmitted and decrease HIV/AIDS. When women are able to plan their families, they are more likely to be able to pursue education, participate in the workforce, and engage in other activities that can improve their economic and social status.
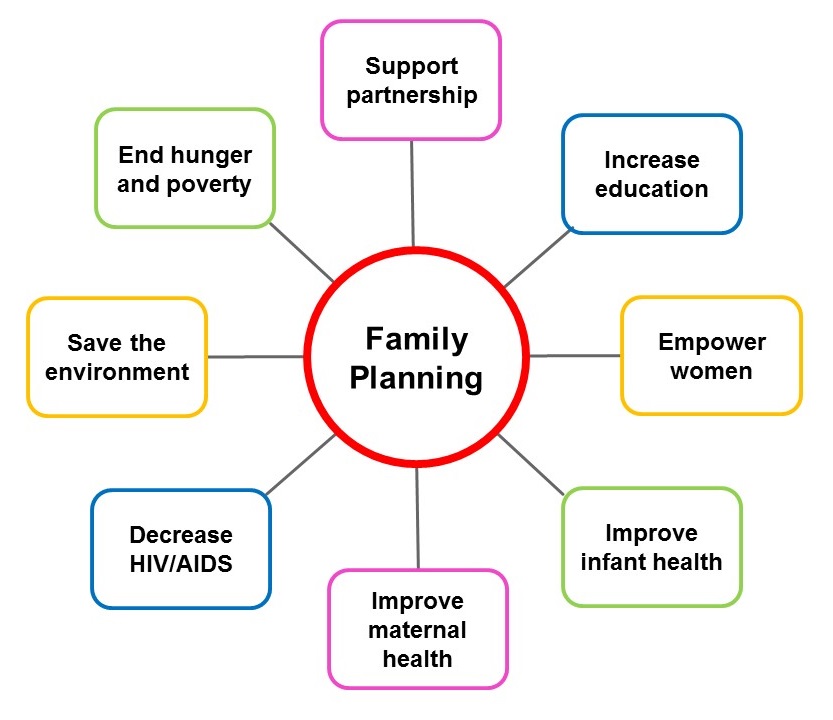
Figure 1 illustrates some of the benefits of Family Planning. Click on image to enlarge
According to a study carried out by Mario Mandara in Nigeria, the use of family planning is influenced by place of residence, age, geographic zone, education, and the number of living children a woman has. Urban women are almost 3 times more likely than their rural counterparts to use a contraceptive method (26% compared with 9%, respectively).
In general, the reproductive age range for women is considered to be between 15 and 49 years old. However, in Nigeria, the average age of first childbirth is around 20-24 years old, and many women may continue to have children well into their 30s and even 40s.
According to the World Bank, as of 2021, the estimated female population of reproductive age (15-49 years) in Nigeria is approximately 53.7 million. This makes up a significant portion of the country's total population, which is estimated to be around 211 million as of 2021.
In Nigeria, a woman of reproductive age is typically defined as a female between the ages of 15 and 49 years old. This is the age range during which women are most likely to conceive and give birth to children. The age range of 15-49 years old is used as a guideline for family planning and maternal health interventions in Nigeria, as well as for data collection and monitoring of reproductive health indicators.
The trends and determinants of fertility in Nigerian women are complex and influenced by a range of social, economic, and cultural factors.
Some of the key trends and determinants of fertility in Nigerian women include:
1. Early marriage and childbearing: Early marriage and childbearing are common in Nigeria, particularly in rural areas and among certain ethnic groups. This can lead to higher fertility rates, as women who marry and have children at a younger age may have more opportunities to have additional children over their reproductive lifespan.
2. Lack of access to family planning: Despite efforts to improve access to family planning in Nigeria, many women still lack access to contraceptives and other reproductive health services. This can contribute to higher fertility rates, as women may have more unintended pregnancies and be unable to space their pregnancies as desired.
3. Cultural and religious beliefs: Cultural and religious beliefs can also influence fertility in Nigerian women. For example, some cultures may place a high value on large families or view contraceptive use as taboo or immoral. Religious beliefs may also discourage contraceptive use or promote traditional gender roles that limit women's control over their reproductive health.
4. Education and socioeconomic status: Education and socioeconomic status are important determinants of fertility in Nigerian women. Women with higher levels of education and income are more likely to have lower fertility rates, as they may delay marriage and childbearing and have more opportunities to access family planning services.
5. Maternal and child health: Maternal and child health indicators, such as infant mortality and maternal mortality, can also influence fertility rates in Nigerian women. High levels of infant and maternal mortality may lead women to have more children in order to ensure that they have surviving children and heirs.
6. Fear of side effects and partner disapproval: Misconception about side effects and partner disapproval may also discourage contraceptive use in Nigerian women.
7. Low awareness of and support for contraceptive use among friends or family: These have also been shown to be additional reasons why contraceptive use in Nigeria is so low.
8. Poor availability of information in the public space: Inadequate public health information and awareness raising over the media, in health facilities, religious centres, etc., may play a role in the low uptake of contraceptive use among Nigerian women.
An introspective look into the local culture of the Nigerian society supports the view that the high fertility rate in Nigeria can be attributed to:
Awareness of family planning (FP) in the Nigerian community has increased over the years, but there are still gaps in knowledge and access to FP services. According to the 2018 Nigeria Demographic and Health Survey (NDHS), 63% of married women in Nigeria reported being aware of at least one modern method of family planning, which is an improvement from 49% in 2013. However, awareness levels vary significantly by region, with higher levels of awareness in urban areas and among women with higher levels of education and income.
Additionally, there are still challenges in accessing family planning services, including limited availability of services in some areas, shortages of trained healthcare providers, and high costs of contraceptives.
Attitudes towards family planning in Nigeria vary widely among women and their partners, and are influenced by a range of factors including culture, religion, education, and socioeconomic status. Here are some common attitudes towards FP in Nigeria:
1. Positive attitudes: Many women and their partners have positive attitudes towards FP, recognizing its importance in promoting reproductive health, preventing unintended pregnancies, and improving maternal and child health outcomes.
2. Negative attitudes: Negative attitudes towards FP are also common in Nigeria, particularly among certain cultural and religious groups that view contraceptive use as taboo or immoral. Some women may also have concerns about the safety and effectiveness of contraceptives or fear side effects.
3. Lack of awareness: Despite increasing awareness of FP in Nigeria, there are still many women and their partners who lack knowledge about the range of available methods and how they work.
4. Fear of side effects: Fear of side effects is a common barrier to FP use in Nigeria, with many women and their partners hesitant to use contraceptives due to concerns about weight gain, mood changes, or other potential side effects.
5. Partner involvement: In many cases, a woman's partner plays a significant role in her decision to use FP. Some men may be supportive of FP and encourage their partners to use contraceptives, while others may be hesitant or even opposed to the idea.
Planned pregnancies spaced two or more years apart result in healthier babies and fewer medical problems for the woman. Planning for a child will help you avoid the social, health, and financial problems you face if an unplanned pregnancy happens.
A study carried out by Agbana et al (2023) reported that 29% of married women use a modern method of FP for child spacing and birth control, whereas 5% use a traditional method. Traditional family planning methods, if used correctly and according to instructions, can be 90% effective but it is considered unreliable.
Modern methods of FP include a variety that are designed to fit the use of women and their partners regardless of biological /physiological features, social status, level education, and sexual lifestyle.
They can be divided into 4 classes as follows:
This is a surgical procedure that makes a person who can produce sperm unable to cause a pregnancy or a person who can ovulate unable to become pregnant.
Permanent birth control is not reversible and prevents pregnancy 99% of the time. While women can choose from bilateral tubal ligation in the hospital (a.k.a “having your tubes tied”) or a tubal block done in a health center, men may choose a vasectomy.
Pros:
Cons:
These work just as the name implies. They are of two types, and involve the use of an Intrauterine Device or Hormonal Implants.
An intrauterine implant is a small t-shaped device that is placed inside of the uterus by a health care provider to prevent pregnancy 99% of the time. Less than 1 out of 100 women will get pregnant each year if they use an IUD.
Pros:
Cons:
Hormonal implants - The implant, which lasts for 3 years, releases the hormone progestin to stop the ovaries from releasing eggs, and it thickens cervical mucus, so it is difficult for sperm to enter the uterus or an egg from fertilizing. It could be in the form of an implant under the skin in your arm that works for 3 to 5 years or injectable contraceptives.
Pros:
Cons:
Barrier methods stop sperm from entering the vagina. The two barrier methods are condoms. These are available for both females and males. Condoms protect against sexually transmissible infections (STIs) and from unintended pregnancy.
Pros:
Cons:
The emergency contraception option is the emergency contraceptive pill (ECP).
ECP is a pill that can be taken up to three days after unprotected sex.
Pros:
Cons:
The best family planning method is the one that most effectively prevents pregnancy and fits with your lifestyle. When you talk with your FP provider and obtain reliable information that helps you to answer the following questions to your satisfaction, you will be better served to decide on a family planning method of your choice.
WHO suggests that you should begin discussing family planning during pregnancy, particularly during the third trimester, after birth and in the immediate postpartum period.
The Nigerian Government provides contraceptives and other family planning commodities at no cost. These services can be accessed at primary health care centres and general hospitals for free.
In summary, family planning is regarded as an essential component of reproductive and general health of women. It can also improve maternal and infant health, promote gender equality, reduce poverty and bolster economies and contribute to sustainable development by empowering women to complete their education, join the paid labour force, be more productive in their jobs, earn higher incomes, increase savings and investment among families. Its uptake should be widely supported and promoted and made part of public health policy.
On a scale of 1-5 (1 being very low, 2 = moderately low, 3 = neutral, 4 = high and 5 = very high), how resourceful was this article to you? Respond and comment here.
REFERENCES
Agbana, R D., Turnwait O. M.,Tolulope F. Ojo, (2018) Family planning method discontinuation among Nigerian women: Evidence from the Nigeria Demographic and Health Survey, Journal of Taibah University Medical Sciences, Volume 18, Issue 1,2023, Pages 117-124, https://doi.org/10.1016/j.jtumed.2022.08.003.
Akamike, I.C., Okedo-Alex, I.N., (2020) Why does uptake of family planning services remain sub-optimal among Nigerian women? A systematic review of challenges and implications for policy. Contracept Reprod Med 5, 30. https://doi.org/10.1186/s40834-020-00133-6.
World Health Organization. Contraception sheet. Last updated 2015 Feb. Accessed April 3, 2023.
World Health Organization Counselling for Maternal and Newborn Health Care: A Handbook for Building Skills. Geneva, 2013. 12, FAMILY PLANNING COUNSELLING.
Mandara, M. (2012) Family planning in Nigeria and prospects for the future. International Journal of Gynecology & Obstetrics.Volume 117, Issue 1, Pages 1-4, ISSN 0020-7292, https://doi.org/10.1016/j.ijgo.2012.01.002.
Alo, O.D., Daini, B.O., Omisile, O.K. et al. Factors influencing the use of modern contraceptive in Nigeria: a multilevel logistic analysis using linked data from performance monitoring and accountability. 2020. BMC Women's Health 20, 191 (2020). https://doi.org/10.1186/s12905-020-01059-6.
The World Bank, World Development Indicators (2012). GNI per capita, Atlas method. [Data file]. Accessed April 8, 2023.
Published: April 27, 2023
© 2023. Datelinehealth Africa Inc. All rights reserved.
Permission is given to copy, use and share content without alteration or modification and subject to attribution as to source.
DATELINEHEALTH AFRICA INC., is a digital publisher for informational and educational purposes and does not offer personal medical care and advice. If you have a medical problem needing routine or emergency attention, call your doctor or local emergency services immediately, or visit the nearest emergency room or the nearest hospital. You should consult your professional healthcare provider before starting any nutrition, diet, exercise, fitness, medical or wellness program mentioned or referenced in the DatelinehealthAfrica website. Click here for more disclaimer notice.


