Labour Induction in Africans: Why, How, Risks and Outcomes
Author: Azuka Ezeike, MB.BS, FWACS (Obstetrics and Gynaecology), FMCOG, MSc. (Public Health). Medically reviewed by: O Oni, MD.

A black pregnant woman wearing a white top and brown pants, sitting with her left hand resting on her bulging belly. Image credit: Freepik
Your doctor just informed you that you will be admitted for the induction of labour, and you are worried. All your sisters and your mother delivered without needing induction, and you are wondering why. You are also worried about the process and whether it is the best option for you.
Labour is a natural process that usually starts on its own in the last weeks of pregnancy. It is common for doctors to wait for this natural process to occur, but on some occasions, there may be a need to start labour artificially. This is usually a well-thought-out and planned process, and your doctor would carry you along throughout.
Induction of labour is the artificial initiation of labour to achieve vaginal delivery [1]. It is recommended if continuing the pregnancy carries more risk for the mother or baby than inducing labour naturally. Pregnancy is expected to last for 40 weeks, but sometimes induction of labour may be needed before 40 weeks or after 40 weeks if labour does not start on its own.
The number of women being induced is rising, especially in Western countries. This is because doctors now understand pregnancy better, and more women either have health problems before pregnancy or develop them during pregnancy.
Because the reasons for induction of labour differ among countries, the rate of induction also differs. Higher rates are observed in Western countries compared to low-income countries. Evidence shows that about 25 out of 100 pregnancies involve the induction of labour in high-income countries. In Nigeria, however, a study reported the rate to be about 3 out of 100 pregnancies.
This article will provide you with information on why and how induction of labour is performed and what to expect during the process.
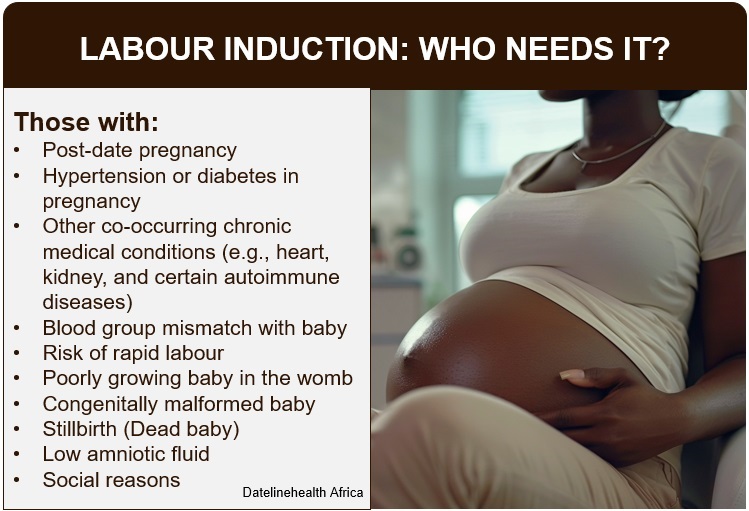
Who needs labour induction? Click on image to enlarge.
The most common reasons for the labour induction include:
The World Health Organization World Health Organization recommends that induction of labour should be carried out if the pregnancy has reached 41 weeks [2]. This is because as pregnancy advances, the placenta becomes weaker, the amniotic fluid reduces, and this may affect the baby.
You may also require induction of labour if you have:
Induction of labour may also be needed if your baby:
Sometimes induction of labour can be done for social reasons, such as: [1]
While induction for a pregnancy that has passed its due date typically occurs around 41 weeks, induction for other reasons may take place earlier, usually between 37 and 39 weeks, depending on the specific condition.

A vial of oxytocin solution, placed beside three white misoprostol tablets and a balloon catheter on a light gray surface. Image credit: ChatGpt
Induction of labour is done using two major methods:
There are two classes of drugs used for the induction of labour. They are:
These are natural substances produced by the body, but they can also be artificially manufactured.
There are two main types:
Prostaglandin E1
Also known as misoprostol. It was originally developed for the treatment of stomach ulcers, but was later found to affect the womb as well. It helps to soften the cervix (the mouth of the womb) and can also induce contractions.
Prostaglandin E2
Also known as dinoprostone. It may come in the form of:
Because they are expensive, prostaglandin preparations other than misoprostol may not be a good option in low-resource settings due to cost and limited access.
Oxytocin is a natural hormone produced in the brain. It can also be produced artificially and is very important in the induction of labour. It helps the muscles of the womb contract. It is usually given as an injection, which is added to an intravenous drip, and administered in drops.
Mechanical methods involve the use of devices or procedures to help soften and open the cervix. They also stimulate the release of prostaglandins, which play an important role in initiating labour.
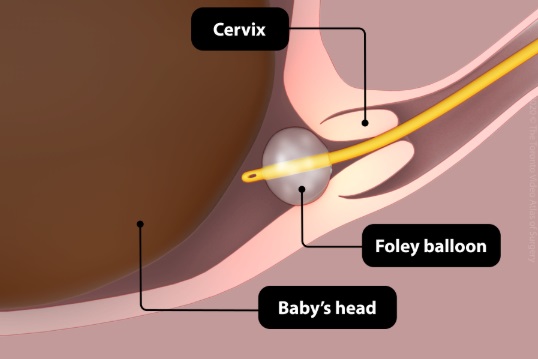
Transcervical balloon catheter method of labour induction. Image credit: TVASurg
This method uses catheters that contain a balloon. The most commonly used one in Africa is the Foley catheter [3]. Originally designed for use in the bladder, it has been adapted for the induction of labour.
Other specialised catheters, such as the Cook’s catheter and double-balloon catheter, exist but are not always available in many African countries.
The procedure involves passing the catheter through the vagina and into the cervix. The balloon is then inflated with water and left in place for about 12 hours. The pressure from the balloon helps soften and dilate the cervix.

Dilapan-S progressive cervical osmotic dilators. Image credit: AJOG-MFM
These dilatators work by absorbing fluid from the cervix, causing them to swell and exert pressure that leads to cervical dilatation. They are also known as osmotic dilators.
They include:
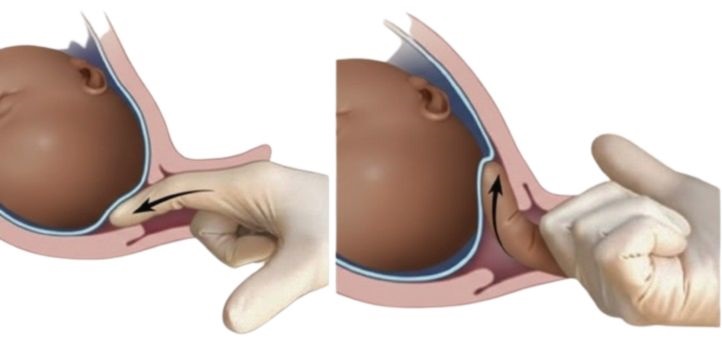
Labour induction by membrane sweeping. Image credit: AJOG-MFM
This procedure is usually performed by a healthcare provider. The doctor inserts a finger into the cervix and gently separates the amniotic sac (bag of water) from the wall of the lower uterus. This process releases prostaglandins, which can help initiate labour.
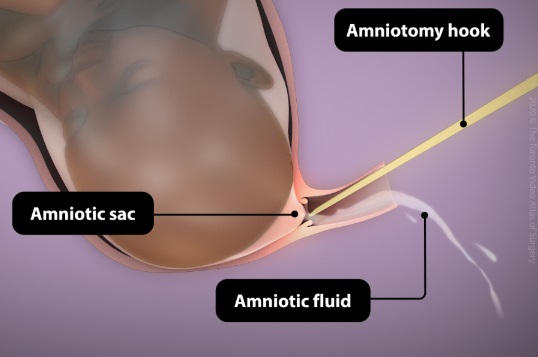
Labour induction through artificial rupture of membrane (Amniotomy). Image credit: TVASurg
Amniotomy is the deliberate rupture of the membranes by the doctor. It is usually done once the cervix has opened sufficiently to make the membranes accessible.
It can be performed:
Amniotomy is rarely used alone for the induction of labour [4].
Your doctor will carry out a quick assessment to confirm you are a good candidate for induction of labour.
This involves:
Cervical ripening is usually started in the evening.
If you have had a previous operation on your womb, such as a caesarean section or fibroid surgery, your doctor will avoid prostaglandins, and in some cases, induction of labour may be avoided altogether.
Induction is usually done using oxytocin.
Throughout the induction, your doctor and midwives will monitor:
This ensures that both you and your baby remain safe during the process.
When induction of labour is properly planned and carried out under medical supervision, it can lead to:
Labour induction is generally safe when closely monitored, but there are some risks. These risks may result from the drugs used (such as oxytocin or prostaglandins) or from mechanical methods [1].
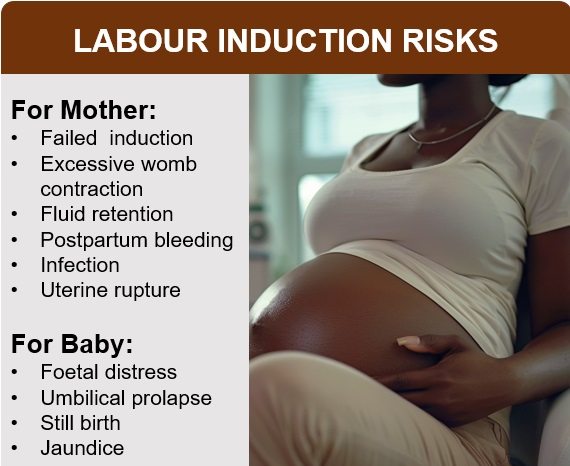
Labour induction risks for mother and baby. Click on image to enlarge.
Conclusion
Labour induction is usually recommended when your doctor believes that continuing the pregnancy may carry more risks than benefits for you or your baby. With proper assessment and close monitoring, induction is generally safe and effective. While there are possible risks, your healthcare team is trained to manage them and keep you and your baby safe.
Induction of labour involves the use of medicines or mechanical methods that may sometimes carry risks for your baby. However, with close monitoring by your doctor and midwives, it is usually safe.
The duration of induced labour can be hard to predict because it depends on how your body responds to the medicines. In most cases, it does not last longer than 48 hours.
The contractions caused by the medicines used for induction may feel more painful than natural labour. However, pain relief options are available during labour to help make you more comfortable.
1. Jenkins SM, Van Hook JW. Induction of labour. [Updated 2023 Feb 20]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 [Cited 2025 Sep 23]. Available from here.
2. WHO recommendations on induction of labour, at or beyond term. Geneva: World Health Organization; 2022. Licence: CC BY-NC-SA 3.0 IGO Available from here.
3. Alu F, Nwachukwu CND, Igbinovia I, Abdulkareem RB, Mai AM, Otubu JAM. Patterns and obstetric outcomes of induction of labour in a public district hospital in Abuja, North Central Nigeria: a five-year review: induced labours and obstetric outcomes in a district hospital. Tropical Journal of Obstetrics and Gynaecology 2024 Jun 19;42(3):195–201. Available from here.
4. Bricker L, Luckas M. Amniotomy alone for induction of labour. Cochrane Database Syst Rev. 2000;2000(4):CD002862. doi: 10.1002/14651858.CD002862. Available from here.
5. Wormer KC, Bauer A, Williford AE. Bishop score. [Updated 2024 Jul 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 [Cited 2025 Sep 25]. Available from here.
6. Wheeler V, Hoffman A, Bybel M. Cervical ripening and induction of labour. Am Fam Physician. 2022 Feb;105(2):177–86. Available from here.
Related:
Essential Guide to Labour for African Women and Men
How to Boost Positive Childbirth Experience in African Women
Oxytocic Drugs in Pregnancy and Labour: An Explainer for Africans
Published: October 21, 2025
© 2025 Datelinehealth Africa Inc. All rights reserved.
Permission is given to copy, use, and share content freely for non-commercial purposes without alteration or modification and subject to source attribution.
DATELINEHEALTH AFRICA INC., is a digital publisher for informational and educational purposes and does not offer personal medical care and advice. If you have a medical problem needing routine or emergency attention, call your doctor or local emergency services immediately, or visit the nearest emergency room or the nearest hospital. You should consult your professional healthcare provider before starting any nutrition, diet, exercise, fitness, medical or wellness program mentioned or referenced in the DatelinehealthAfrica website. Click here for more disclaimer notice.


