Myomectomy – The Fibroid Surgery African Women Need to Know
By Udochukwu Glory Maduka, MB.BS. Medically reviewed by: Azuka Ezeike, MB.BS, FWACS (Obstetrics and Gynaecology), FMCOG, MSc. (Public Health).

A young Afro woman wearing eyeglasses and a beige t-shirt, in apparent pain and holding on to her abdomen. Chronic pain in the lower belly is one of the reasons for myomectomy in women who are known to have fibroids. Image credit: Freepik
Fibroids are one of the most common health concerns among African women, especially those in the reproductive age (between 25 and 45 years).
They are abnormal growths, usually non-cancerous (benign), that arise in the muscles of the uterus (womb).
They come in different sizes- the small and large ones. And can present with some symptoms, such as heavy menstrual bleeding, etc. depending on the location.
Black women face the highest risk of this condition, with rates 3 to 4 times higher than women of other races. It is estimated that 70 to 80% of black women will develop fibroids in their lifetime. [1]
Myomectomy (surgical removal of fibroids) offers a solution that removes the fibroids while preserving the uterus for women who want to bear children.
In this guide, we’ll explain who needs this surgery, how to prepare for it, what to expect during and after the procedure, and possible risks.
Myomectomy is a type of surgery done to remove fibroids from the uterus (also known as the womb) while preserving the tissues of the uterus to enable the woman to still get pregnant after the surgery.
It is different from a hysterectomy, which is a surgery done to completely remove the uterus (womb), in which case, the woman can no longer carry a pregnancy.
Abdominal myomectomy
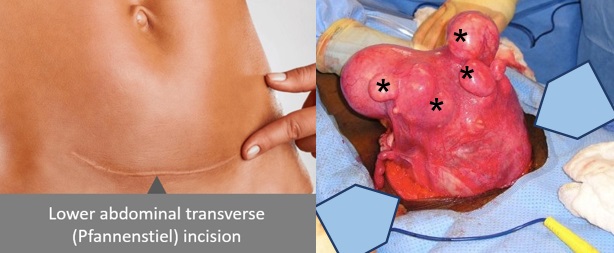
Fig. 2: Showing composite illustration of Pfannenstiel (bikini) incision in the lower abdomen of a woman (L) and multiple uterine fibroids from an open myomectomy.(R). Click on image to enlarge.
Abdominal myomectomy is also known as open myomectomy (see fig. 2). It is usually used to remove fibroids (leiomyomas) of any size, but typically large ones that are located in the muscle and underneath the outer walls of the uterus and causing several complications (see fig. 1).
The surgery involves the following steps: [2]
Short term recovery takes 3 to 5 days in the hospital and 4 to 6 weeks to return to work.

Fig. 3: Illustration of a typical operating scene during laparoscopic myomectomy. Image credit.
This type of myomectomy may be right for you if you have a few and small-sized fibroids that are located beneath the outer covering of the uterus (see fig 1). In well experienced hands, laparoscopic myomectomy may be used to remove large fibroids too. [3, 4] The fibroids are removed through small cuts in your abdominal (belly) wall in a procedure that is identified as minimally invasive surgery. The surgical procedure involves the following steps: [2]
Compared to open myomectomy, laparoscopic myomectomy causes less bleeding, has fewer complications, and leaves less scar tissue. You will recover in the hospital faster—typically in 1 to 2 days. [4]
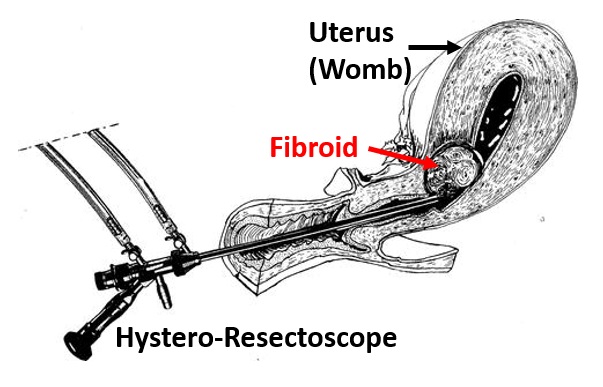
Fig 4: Cartoon illustration of a hysteroscopic myomectomy. Click on imge to enlarge. Image credit
This procedure is another minimally invasive surgery for removal of fibroids. It is best suited for the removal of a fibroid that grows into the cavity of the uterus (womb). This type of fibroid is called submucosal fibroid (see fig. 1). It does not require any incision on the abdominal wall. The procedure involves: [2]
Hysteroscopic myomectomy is a day procedure, and you can go home after full recovery from the GA.
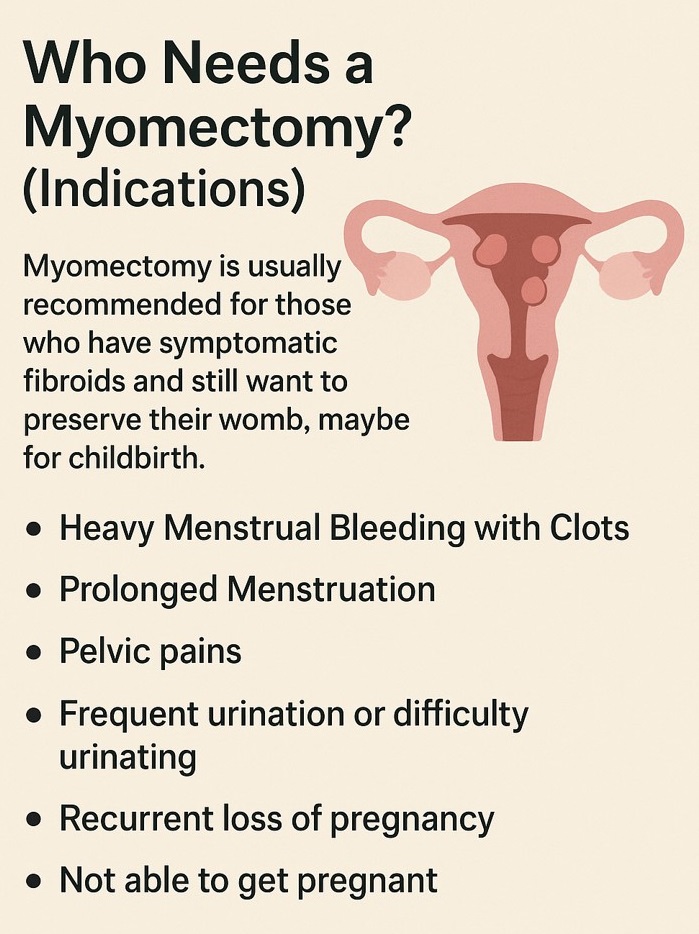
Fig. 5: Indications for myomectomy. Click on image to enlarge.
Myomectomy is usually recommended for those who have symptomatic fibroids and still want to preserve their womb, maybe for childbirth (see fig. 5). Symptomatic fibroids are fibroids that are causing noticeable symptoms, such as:
When meeting with your doctor to discuss the surgery, take the opportunity to ask any questions you may have about preparation and what you can expect throughout the process.
Your doctor will likely recommend imaging tests, such as an ultrasound or Magnetic Resonance Imaging (MRI), to effectively determine the location, size, and number of fibroids.
Blood tests will also be beneficial in assessing anaemia, ensuring proper clotting, and evaluating your overall health.
Arrange to make blood available. This is because myomectomy may be associated with blood loss that could require transfusion. Your husband or any relative can donate. The amount of blood needed is determined by your doctor.
Your doctor will further explain the surgery and give you an informed consent form to sign. Be sure to read the form carefully, ask questions on any content of the form that you do not understand or are unsure about before signing it. You can also ask your husband or a family member to read and sign the form on your behalf.
In preparation for the surgery, it’s important to share all medications you currently take, including vitamins and supplements, with your doctor, as some may need to be paused before your myomectomy. [5]
If you smoke, try to quit six to eight weeks before your surgery. This can help you heal better and decrease your risk of heart problems. Your doctor can support you in this effort.
You will stop eating and drinking after 10 pm before your surgery to ensure the best possible outcome.
Before the surgery starts, you will be given anaesthesia so you won’t feel pain.
The type of anaesthesia depends on the type of myomectomy. It may be general, spinal, epidural, or a mix of spinal and epidural types called Combined Spinal Epidural (CSE). [4]
This puts you into a deep sleep during surgery, with a tube placed in your throat for breathing. Commonly used for laparoscopic, robotic, and abdominal myomectomies, and sometimes for hysteroscopic myomectomies.
A single injection into the spinal fluid so you stop feeling your lower body. It is sometimes used for abdominal myomectomies and can be combined with epidural anaesthesia.
A catheter is placed near the spinal cord (in the epidural space) to deliver pain medication, providing relief during and after abdominal myomectomies.
It merges spinal and epidural techniques for quick pain relief and prolonged comfort.
This helps you relax and feel drowsy without using a breathing tube. The anesthesiologist stays with you during a procedure, continuously monitoring vital signs (like heart rate, breathing, blood pressure, oxygen levels) and adjusting medications as needed. It is often used for less invasive procedures like hysteroscopic myomectomies.
After you have received anaesthesia, the surgeon will make a careful incision based on the chosen surgical method.
The fibroids will be removed, and your uterus will be properly sutured back afterwards depending on the type of myomectomy performed.
Sometimes, a drainage tube is passed from inside your abdomen to the outside to help drain fluids (blood) accumulating inside after the closure depending on the surgeon and extent of surgery.
The whole procedure usually takes about 1 to 3 hours, depending on how many fibroids there are and their size.
Expect a recovery period of 4 to 6 weeks for open surgery and 2 to 4 weeks for minimally invasive surgery.
You can conceive after undergoing myomectomy, but doctors usually recommend waiting 3 to 6 months before attempting to get pregnant.
Fibroids can sometimes regrow, so regular follow-up care is essential.
Taking care of yourself after surgery can help reduce these risks.
Myomectomy is a safe and effective way to treat fibroids while preserving fertility. If you have fibroid-related symptoms that are affecting your quality of life, talk to your gynaecologist about whether this procedure is right for you.
Can I get pregnasnt after myomectomy?
Yes, many women go on to have successful pregnancies after the surgery.
Will my fibroids come back?
They can, especially in younger women, but recurrence rates vary.
Is myomectomy safer than hysterectomy?
It’s generally considered safer for women who want to still have children after the surgery, but every case is different.
How soon can I return to work?
Light office work can resume in 2–4 weeks for minimally invasive surgery; 4–6 weeks for open surgery.
1. Igboeli P, Walker W, McHugh A, Sultan A, Al-Hendy A. Burden of Uterine Fibroids: An African Perspective, A Call for Action and Opportunity for Intervention. Curr Opin Gynecol Obstet. 2019;2(1):287-294. doi: 10.18314/cogo.v2i1.1701. Available from here.
2. UCSF Health. Myomectomy [Internet, n.d.]. San Francisco (CA): UCSF Health; [cited 2025 Aug 22]. Available here.
3. Asaolu OA, Ejenobo DTE; Alabi OA. Laparoscopic Myomectomy for Huge Uterine Fibroid in Sub-Saharan Africa: A Case Report. African Journal of Reproduction and Gynaecological Endoscopy 2023;8(1):p 32-36. doi: 10.4103/ajrge.ajrge_9_23. Available from here.
4. Barjon K, Kahn J, Singh M. Uterine Leiomyomata. [Updated 2025 May 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. [Cited August 29, 2025] Available from:here.
Related: Fibroid; What Every African Woman Should Know
Published: August 30, 2025
© 2025. Datelinehealth Africa Inc. All rights reserved.
Permission is given to copy, use and share content without alteration or modification and subject to source attribution.
DATELINEHEALTH AFRICA INC., is a digital publisher for informational and educational purposes and does not offer personal medical care and advice. If you have a medical problem needing routine or emergency attention, call your doctor or local emergency services immediately, or visit the nearest emergency room or the nearest hospital. You should consult your professional healthcare provider before starting any nutrition, diet, exercise, fitness, medical or wellness program mentioned or referenced in the DatelinehealthAfrica website. Click here for more disclaimer notice.


