Heartburn and Acid Reflux Explained to Africans: Symptoms and Treatment
By Oluwasola Samuel, Freelance health writer. Medically reviewed by A. Odutola. MB BS, PhD, FRCSEd
October 26, 2025
An AI generated image of an African man wearing a grey T-shirt. He's holding his chest in pain probably from heartburn, caused by acid reflux.
You may hear people talking about "heartburn" and "acid reflux" as if they mean the same thing. Also, some people think heartburn has something to do with the heart. But these are not true. Although associated, heartburn is different from acid reflux and it has nothing to do with the heart.
Heartburn is a burning sensation or pain that you feel in your chest. It is commonly caused by acid reflux.
Acid reflux, on the other hand, is the movement of the acidic content of your stomach upwards into your oesophagus (the gullet or food pipe or tube that connects your throat to your stomach) through a weak “control valve” called the lower oesophagus sphincter (see fig. 1).
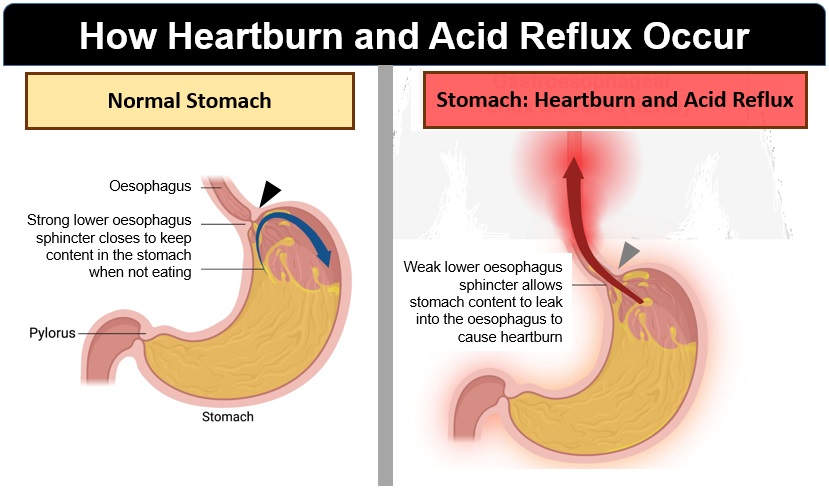
Fig. 1: Illustration showing how heartburn and acid reflux occur. Click on image to enlarge.
When acid reflux occurs chronically (i.e., for a long time), it causes a condition called Gastroesophageal Reflux Disease or GERD.
Acid reflux may occur soon after you eat a rich, acidic, or spicy meal, bend over after a meal, or when you lie down too soon after a meal. This upwards movement of stomach acid most times irritates and causes the lining or wall of your oesophagus to swell and get inflamed. This condition (swelling and inflammation of the wall of the oesophagus) is known as oesophagitis. (1)
In this article, you will learn about heartburn and acid reflux from these viewpoints:
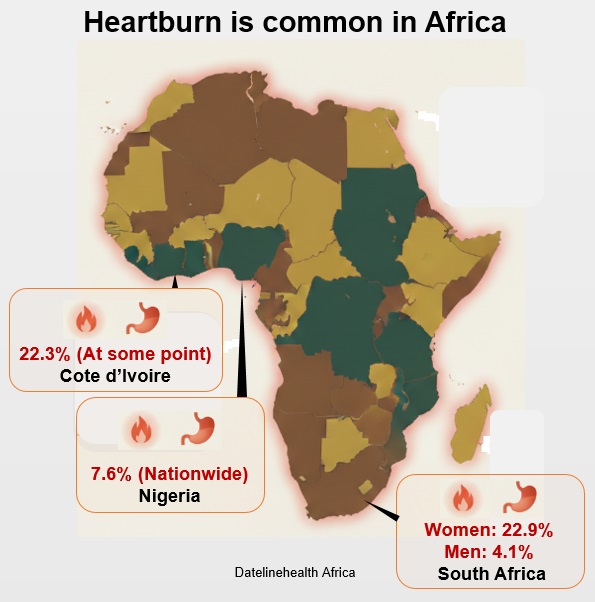
Fig. 2: Map showing heartburn prevalence in Nigeria, Cote d'Ivoire or Ivory Coast, and South Africa. Click on image to enlarge.
Heartburn is more common in Africa than most people think. It's not just a “Western” problem; it also affects Africans (see fig. 2).
In Nigeria, a study found that around 7.6% of people said they often felt a burning sensation in their chest region. (2) Another research in Abidjan (Ivory Coast) reported that about 22.3% of people reported feeling heartburn at some point and about 9.2% said it happens at least once every week. (3) Also in Nigeria, studies carried out in the Southwestern part of the country have shown higher figures, ranging from 9.3% to 36%. (4)
In South Africa, a study in a black adult population showed heartburn symptoms were reported in about 22.9% of women and 4.1% of men. (5) Taken together, these numbers would suggest that heartburn is common in different African countries.
Large and well controlled studies are still needed to understand the occurrence of heartburn and acid reflux between rural and urban African populations and the differences between countries across Africa. Without this broader data, we are likely to underestimate how widespread heartburn is in Africa.
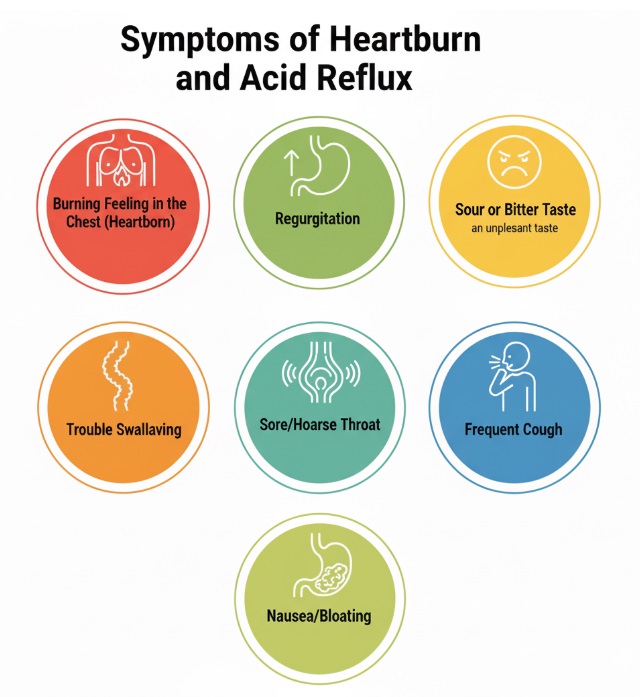
Fig. 3: Infoposter showing some symptoms of heartburn and acid reflux; feelings of burning in the chest, regurgitation, sour taste in the mouth, trouble swallowing, sore throat, frequent cough, nausea, bloating. Click on image to enlarge.
If you or your loved ones often feel a burning sensation or notice discomfort after eating, you need to pay attention.
Below are some common symptoms of heartburn and acid reflux. Also see fig. 3.
The burning feeling in your chest usually happens after eating or when you lie down. This burning feeling can feel like fire rising from your stomach up towards your throat.
You might belch (a loud gas released from your stomach through your mouth) up some food or liquid after eating. This food or liquid comes back up to your throat in small amounts. This symptom is different from vomiting.
You may feel food coming back up, leaving a bitter or sour taste. This happens because the acid from your stomach travels up your oesophagus to reach your mouth.
You may feel like food is stuck in your throat or chest. This happens when the stomach acid that escapes from your stomach causes irritation and slightly narrows your oesophagus over time.
When acid escapes from your stomach, it can irritate your throat especially at night. This can leave your throat dry or make your voice sound off or rough.
As stomach acid irritates and makes your throat dry, it can cause coughs that don't go away easily.
You may feel fully gassy or slightly sick immediately after your meal. That's a sure sign of acid reflux.
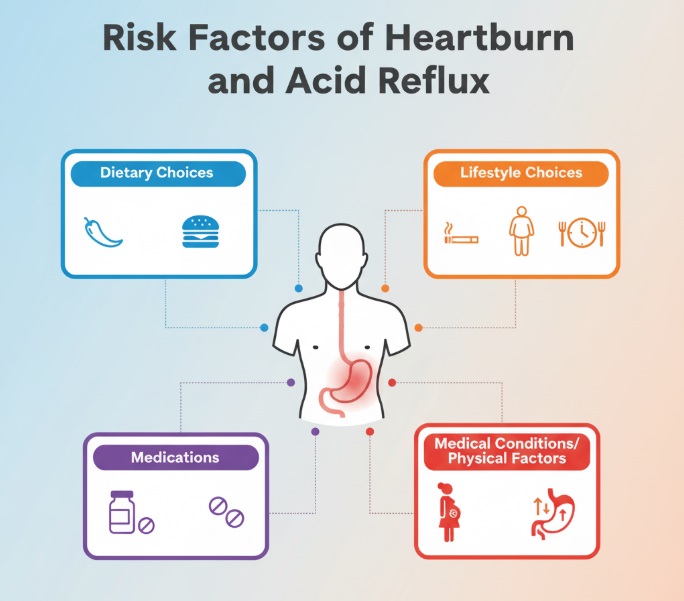
Fig. 4: Risk factors of heartburn and acid reflux. Click on image to enlarge.
Certain factors that put you at risk for heartburn and acid reflux include (see fig. 4):
Dietary choices have to do with your choice of meals or eating habits. Some risk factors under dietary choices include:
This has to do with medical conditions and physical factors you cannot control.
Some of these risk factors include:
Certain medications can relax the lower oesophageal sphincter (LES), to allow stomach acid to escape your stomach into your oesophagus, causing heartburn. (6) Some of these medications include the following:
This includes activities you indulge in that increase your risks. Some of these include:
If you often feel a burning sensation in your chest that interferes with your daily life or you are always reaching for antacids, it is time you see your doctor or other healthcare professionals (HCP). (7)
Most times your symptoms alone tell the story. But if symptoms are frequent and interfere with your daily life, your healthcare professionals (HCP) will evaluate you further.
These would likely include:
Your doctor will ask about your symptoms:
Your doctor may also ask about your diet, lifestyle and the medications you take. In most cases, in the African healthcare setting, if your responses and symptoms point to acid reflux, your doctor may tentatively diagnose this condition and start treatment immediately without further evaluation.
If your doctor has some concerns about other diagnosis besides heartburn/acid reflux, they could put you on heartburn medication(s) for a trial period to evaluate your response to them or request that you undergo further laboratory tests that may include:
If your symptoms don't improve following the medication trial, your doctor may recommend an endoscopy test. An endoscopy is a procedure or test that involves the use of an endoscope (a thin, flexible tube with a camera at its tip). This flexible tube is gently guided through your mouth and into your oesophagus.
While the endoscope is in your oesophagus, it allows your doctor to have a visual image on screen of what's happening (redness, swelling, or signs of severe damage) there. Your doctor may take a biopsy (small tissue sample) of the lining of your oesophagus for lab testing.
This test is carried out to ascertain or measure the amount of acid in your oesophagus. To carry out this test, your doctor would carefully insert a catheter (a thin, flexible tube with a pH sensor) through your nose into your oesophagus. The other end outside is connected to a recording device that's attached to your belt or a strap around your waist.
Here, the sensor at the tip of the catheter, carefully guided into your oesophagus, measures acidity levels and transmits data to the recorder.
This test measures muscle activity in your oesophagus as you swallow. (8) Here, you will be required to sit upright while your doctor or another health care provider carefully passes a catheter through your nose into your oesophagus.
At this point, you will be asked to drink sips of water frequently. While swallowing, the sensor on the catheter records the pressure generated by the muscles on the wall of your oesophagus. This procedure may also help your doctor in making appropriate diagnosis of your condition.
5. Oesophagram
This examination is a simple imaging test that shows the shape and movement of your oesophagus and stomach. (9) To carry out this diagnosis, a radiologist (a specially trained doctor who specialises in using medical imaging to diagnose and treat diseases) gives you a substance called barium (a whitish substance that coats the inside of your oesophagus and stomach) to drink. This substance outlines your upper digestive tract and reveals any abnormalities during the X-ray.
Not everyone needs all these tests. Your doctor would advise you on the tests that are appropriate for you based on your symptoms.
The good news about heartburn and acid reflux is that they can be treated. (10) In many cases, simple lifestyle changes can make a big difference. However, if symptoms are frequent or severe, your doctor may recommend medication or in rare cases, surgery.
The treatment options can be divided into:
1. Lifestyle changes
After receiving a diagnosis of heartburn and acid reflux, you doctor may be asked to try some lifestyle changes to help improve your symptoms.
Below are some of the lifestyle changes:
To prevent acid reflux, eat smaller portions of food. When you eat in smaller portions, your stomach is not overstretched, and it will not produce too much acid during digestion.
If you must lie down, wait at least 3-5 hours after a meal before going to bed. By this time, most of the food you eat must have been digested, which reduces your risk of acid reflux.
Abdominal pressure is a contributory factor to acid reflux. Avoid wearing tight clothing, belts, or waistbands before, during, or after meals.
Some foods trigger or increase the production of acid in your stomach. Some of the main triggers are:
Ensure you keep a diary to note which food triggers your symptoms.
Cigarettes contain harmful chemicals that weaken the lower oesophageal sphincter (LOS) over time. As a result, quitting will help the LOS work properly again.
You may be asked by your doctor to see at a dietician and physiotherapist to help you with diet and exercise plans respectively for the purpose of losing weight if you are overweight or obese.
If lifestyle changes do not improve your symptoms, your healthcare provider may ask you to start taking medications that may include:
Antacids are neutralisers that provide quick relief. It is a neutraliser that makes stomach acid ineffective, making it less corrosive to the oesophagus. However, it doesn't heal the irritation already caused in the oesophagus.
The H2 blockers provide longer relief when compared to antacids. H2 blockers block the chemical (Histamine) that sends signals to the body to produce stomach acid. This disruption can go on for several hours. This is to help reduce the amount of stomach acid produced during specific intervals.
The proton pump inhibitor is a medication mostly used for severe cases. This acid blocker prevents acid from getting into your oesophagus. It also heals damaged tissues in your oesophagus and allows it to recover. Proton pump inhibitors are very effective and widely used.
Surgery is rarely needed to treat acid reflux. However, they can be helpful for people who do not respond to lifestyle changes and medications or have complications. Talk with your doctor to know if surgical treatment is right for you in managing your heartburn and acid reflux problem.
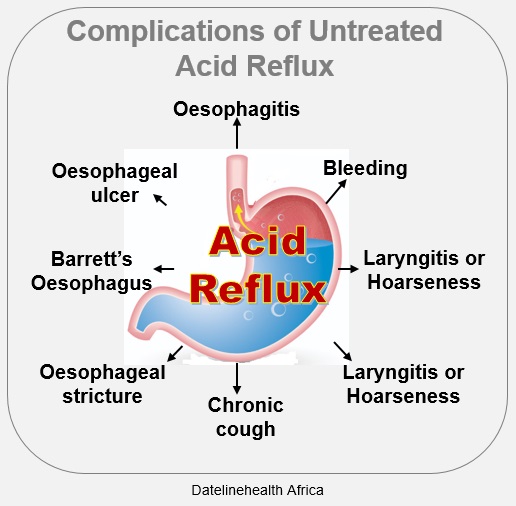
Infoposter on the complications of untreated acid reflux. Click on image to enlarge.
If poorly treated or not treated, acid reflux can lead to complications, including:
It's normal to experience heartburn after a heavy or spicy meal. But when the burning sensation is frequent, or over-the-counter prescriptions are no longer effective, it’s time to visit your doctor.
Below are signs and situations when you should see a doctor:
While most acid reflux cases are easy to treat, untreated ones can damage your oesophagus and increase your risk of more serious conditions like ulcer or even oesophageal cancer over time. So if you notice any signs mentioned above, kindly make an appointment with your HCP.
Heartburn and acid reflux are your body’s way of telling you that something needs to change. They are often triggered by lifestyle habits like eating large meals, lying down too soon after eating, smoking, or drinking alcohol. The good news is that these conditions are treatable and even preventable through simple changes such as eating smaller meals, avoiding trigger foods, quitting smoking, staying active, and maintaining a healthy weight.
However, if heartburn keeps coming back or over-the-counter medicines stop working, it’s time to see your healthcare professional. Ignoring frequent heartburn can lead to serious complications, including damage to your oesophagus. Take charge of your health today. Identify your triggers, make small consistent changes, and seek medical help when needed. Prevention is always easier and safer than treatment.
1. Is heartburn common during pregnancy
Yes, heartburn is a common symptom during pregnancy. Many women experience it for the first time during pregnancy.
Here is what happens: During pregnancy, your body produces more hormones (progesterone) that relax the lower oesophageal sphincter. (11) As a result, acid can escape into your oesophagus causing a burning pain in your chest area. Another way this can also happen is that as your baby grows, the uterus (womb) pushes against your stomach which makes it easier for acid to move up into your oesophagus.
Yes, antacids are generally safe for relieving heartburn. Antacid acts as a neutraliser that makes stomach acid less corrosive to your oesophagus.
No, stress alone may not be a direct cause of heartburn, but it can trigger or worsen heartburn over time.
For mild symptoms of acid reflux, it usually takes a few minutes or a couple of hours. The discomfort often fades away once your stomach is empty or after taking an antacid. However, when acid reflux is severe, it can keep coming back several times a week or last for days.
1, Mayo Clinic. Esophagitis - Symptoms and causes [Internet]. 2024 October 29. [Cited 2025 Oct 19]. Available from here.
2. Nwokediuko SC, Adekanle O, Akere A, Olokoba A, Anyanechi C, Umar SM, et al. Gastroesophageal reflux disease in a typical African population: a symptom-based multicenter study. BMC Gastroenterology. 2020 Apr 15];20(1):107. Available from here.
3, Assi C, Koné S, Ndjitoyap AWN, Ouattara A, Lawson-Ananissoh LM, Djenabou D, et al. Prevalence of heartburn in Abidjan, a black African country, and associated factors. Open Journal of Gastroenterology. 2014 Mar 27;2014. Available from here.
4. Sadiq MA, Abdulmumini Y, Sakajiki AM, Hayatu U, Abdullahi BS, Jibril BA, et al. Endoscopic correlation of clinical presentation of gastroesophageal reflux disease among patients referred for gastroscopy in a tertiary hospital. World Journal of Advanced Research and Reviews. 2020;19];6(2):037–43. Available from here.
5. Hunter MP, Crowther NJ. The prevalence of gastroesophageal reflux disease in an adult, South African black population, and the association with obesity. Minerva Gastroenterol Dietol. 2019 Jun;65(2):100–6. Available from here.
6. Rosen RD, Winters R. Physiology, Lower Esophageal Sphincter. [Updated 2023 Mar 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Retrieved October 19, 2025. Available from here.
7. Salisbury BH, Terrell JM. Antacids. [Updated 2023 Aug 08]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Retrieved October 19, 2025. Available from here.
8. Hopkins Medicine. Esophageal manometry: [Internet, n.d.]. [Cited 2025 Oct 19]. Available from here.
9. Chen A, Tafti D, Tuma F. Barium swallow. In StatPearls. [Updated 2023 Jul 24]. StatPearls Publishing. Retrieved October 19, 2025. Available from here.
10. NIH. National Institute of Diabetes and Digestive and Kidney Diseases. Treatment for GER & GERD? [Internet]. Last update: July 2020. [Cited 2025 Oct 23]. Available from here.
11. Cable JK, Grider MH.. Physiology, progesterone. [Updated 2023, May 01]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Retrieved October 19, 2025. Available from here.
Published: October 26, 2025
© 2025. Datelinehealth Africa Inc. All rights reserved.
Permission is given to copy, use, and share content freely for non-commercial purposes without alteration or modification and subject to source attribution.
DATELINEHEALTH AFRICA INC., is a digital publisher for informational and educational purposes and does not offer personal medical care and advice. If you have a medical problem needing routine or emergency attention, call your doctor or local emergency services immediately, or visit the nearest emergency room or the nearest hospital. You should consult your professional healthcare provider before starting any nutrition, diet, exercise, fitness, medical or wellness program mentioned or referenced in the DatelinehealthAfrica website. Click here for more disclaimer notice.


