Intestinal Obstruction in African Adults
By: Chinwendu Glory Ogbonna. B.Sc. Biochem. Freelance Health Writer and DLHA Volunteer. Medically reviewed by A. Odutola FRCSEd.

Close up of a young African wearing an unbuttoned blue shirt, sitting on a sofa and holding his belly in pain and obvious distress. Image vredit. Freepik
Have you ever felt sharp cramps, bloating, or constant vomiting and wondered, “Have I caught a stomach bug?” That’s often how an intestinal obstruction begins, mimicking common stomach issues in its early stages. But within moments, what seems like mild discomfort can quickly become a serious small or large bowel blockage. Intestinal obstruction is a surgical emergency that can become life-threatening if not diagnosed and treated promptly.
Intestinal obstruction also known as bowel blockage occurs when the small or large intestine is partially or completely blocked, preventing the normal flow of digestive contents. It may be mechanical (physical blockage) or functional (caused by poor intestinal movement). Prompt diagnosis is essential, as the condition can become life-threatening if not treated in time.
This article aims to educate you about intestinal obstruction, a serious digestive condition that can become fatal if ignored. It explains what intestinal obstruction is, its causes, risk factors, and warning signs. You’ll also learn how it’s diagnosed and the available treatment options, ranging from supportive care with wait and watch to planned or emergency surgery.
Before diving deep into intestinal obstruction at length, it's important to understand the basic structure and function of the digestive system, as these help to explain why a blockage in the intestines can be so dangerous.
The gastrointestinal (GI) tract or GIT, also referred to as the digestive system, is a long tunnel of approximately 30 feet or 9 metres, which starts at the mouth and ends at the anus. Much of this long tube that makes up the tunnel is coiled up inside the abdomen (see figure 1).
The basic parts of the GIT include:
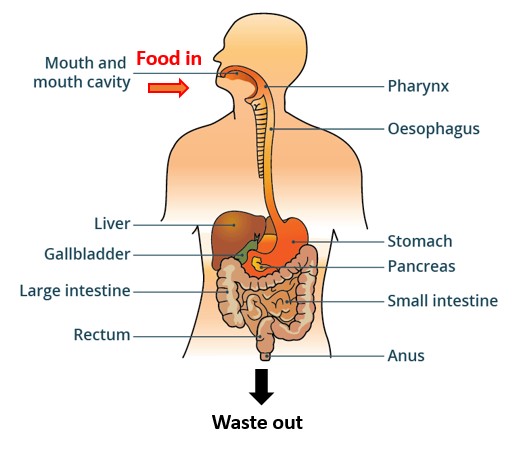
Figure 1: Showing basic parts of the gastrointestinal tract (GIT). Click on image to enlarge.
Several other organs like the liver, gall bladder, and pancreas are associated with the GIT and make up the digestive system. Further consideration of these organs is outside the scope of this article.
The function of the GIT is to digest or break down food, absorb nutrients, and get rid of waste.
The process of digestion starts from the mouth where food is chewed and mixed with juices and enzymes in saliva before it is swallowed into the stomach, through the oesophagus.
The stomach mixes the food with more juices and enzymes before passing the increasingly digested food into the small intestine where further breakdown (digestion) continues and nutrients from the digested food are absorbed into the blood stream to be used for body nourishment, body building, repair and energy.
From the small intestine, what is left after digestion and absorption is passed through the large intestine, where more nutrients and a lot of water are absorbed into the blood stream.
What is then left of the process in the large intestine becomes stool, which is stored partly and temporally in the rectum, the terminal part of the large bowel, before being excreted or pushed out through the anus.
Each part of the connected GIT plays a role in keeping your body nourished and balanced. But when something blocks the flow of food through the tract, especially in the intestines, it can cause serious pain, illness, or worse.
Watch the video below to learn more about the anatomy (structure) of the GIT and see the pathway of food through the tract
Bowel obstruction can result from various issues and arise from either the small or large bowel, especially in adults with surgical history or chronic conditions.
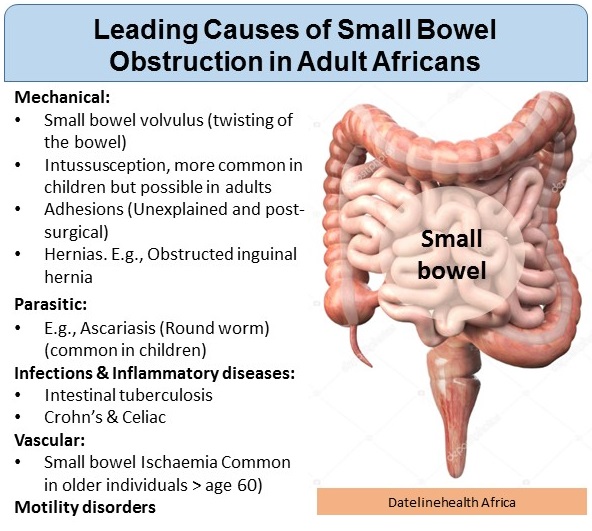
Fig. 1: Showing leading causes of small bowel obstruction in adult Africans. Click on image to emlarge.
The leading causes of small bowel obstruction in Adult Africans (see fig 1) include:
The leading causes of large bowel obstruction in adult African countries (see fig. 2) include:
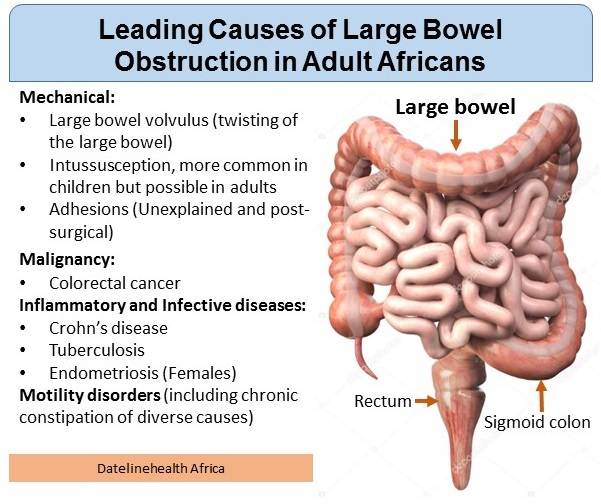
Fig. 2: Showing leading causes of large bowel obstruction in adult Africans. Click on image to enlarge.
Mechanical:
Recognizing early symptoms can save lives. Watch for:
These signs should never be ignored. Early detection and diagnosis can help prevent complications like bowel perforation or sepsis.
Before a diagnosis is made, healthcare providers will take a detailed medical history.
This includes:
Your medical history helps doctors understand the likely cause of the obstruction and decide the next steps for diagnosis and treatment.
Additional processes in your diagnosis journey include:
This involves touching, feeling and using needed tools to check all parts of your body and more especially your abdomen (belly) for any tenderness, bloating, or abnormal bowel sounds
These may include:
Imaging
These tools help doctors determine whether surgery or non-surgical treatment is needed.
Intestinal obstruction is a serious condition of the digestive tract. In African adults, the risk factors for the condition often reflect unique health challenges due to high infection rates, environmental factors and a rise in especially colorectal cancer and other chronic diseases.
In African adults, the common risk factors for intestinal obstruction (see fig. 3) are often also causes of the condition and they include:
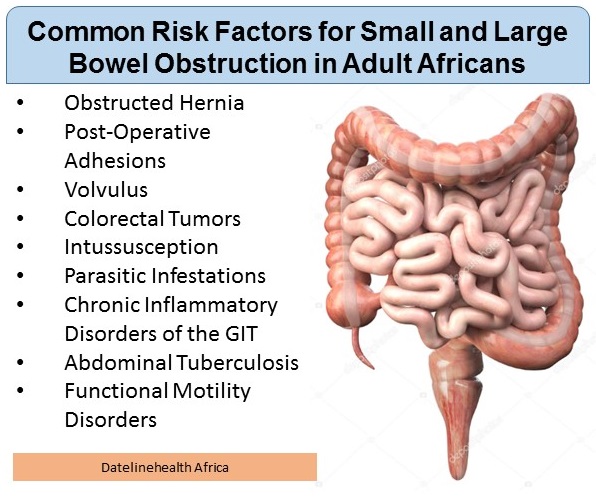
Fig. 3: Showing common risk factors for small and large bowel obstruction in adult Africans. Click on image to enlarge
Hernias, especially inguinal are a leading cause of bowel obstruction in African adults. Untreated hernias can trap parts of the intestine, cutting off blood flow and leading to obstruction. According to a reported study in Sokoto Nigeria, obstructed hernias accounted for 47.9% of adult hospital cases.
Adhesions are bands of scar tissue formed after abdominal surgery that can block the intestines. As more surgeries are done in urban African hospitals, adhesive obstructions are on the rise. A Nigerian meta-analysis across 10 studies found adhesions caused 46.3% of adult small bowel obstructions.
3. Volvulus (Twisting of the Bowel)
Volvulus occurs when a loop of the bowel twists on itself, cutting off blood supply and causing obstruction.
In Uganda, sigmoid volvulus accounts for approximately 20–23.5% of intestinal obstruction cases, as observed in regional hospitals and referral centers across Northern Uganda, including Kampala.
In Ethiopia, sigmoid volvulus is the leading cause of large-bowel obstruction, accounting for up to 69% of cases in some hospitals. A systematic review of Ethiopian hospital recordss confirmed this trend, highlighting its major role in the burden of large-bowel obstruction.
Colorectal cancer, although previously believed to be less common in Africa, now accounts for about 10% of bowel obstruction cases in a small sample of adult hospital admissions in Nigeria. Similar patterns are noted in regions like Ethiopia though locally published data are more limited.
This condition, where part of the intestine folds into another appears in 4-10% of adult African cases.
Heavy Ascaris infestation can create worm boluses that physically block the intestines. This remains a concern in areas with poor sanitation.
People with undiagnosed chronic inflammatory diseases of the bowel, like Crohn's or Celiac disease are at high risk of developing intestinal obstruction. The causes of the conditions are unknown but genetics and environmental factors are believed to play roles.
TB infection of the intestines leads to thickening and narrowing of the bowel, potentially causing obstruction.
Treatment of intestinal obstruction is dependent on the cause and severity.
Surgery is needed if:
Procedures may include:
Timely intervention is crucial to reduce the risk of sepsis or death.
While not all bowel obstructions are preventable, these steps reduce risk:
Recovery doesn’t end after acute treatment:
Know that adhesion-related obstructions recur in patients according to studies. Preventative care, awareness, and timely responses are key to avoiding another emergency.
Bowel obstruction is a critical digestive emergency often mistaken for minor stomach pain. This article urges readers to take symptoms like sudden abdominal pain, vomiting, and bloating seriously and seek immediate medical care. Early detection and treatment are crucial to preventing life-threatening complications. Whether you're a patient, caregiver, or health-conscious individual, this piece empowers you with essential knowledge to recognize the warning signs and act quickly.
About the author::

Chinwendu Glory Ogbonna is a freelance health writer, focused on Africa-centred health and wellness topics. She is passionate about creating relatable and actionable health content for diverse audiences.
Published: July 31, 2025
© 2025. Datelinehealth Africa Inc. All rights reserved.
Permission is given to copy, use and share content for non-commercial purposes without alteration or modification and subject to source attribution.
DATELINEHEALTH AFRICA INC., is a digital publisher for informational and educational purposes and does not offer personal medical care and advice. If you have a medical problem needing routine or emergency attention, call your doctor or local emergency services immediately, or visit the nearest emergency room or the nearest hospital. You should consult your professional healthcare provider before starting any nutrition, diet, exercise, fitness, medical or wellness program mentioned or referenced in the DatelinehealthAfrica website. Click here for more disclaimer notice.


