Why Sickle Cell Disease Burden Remains High In Africa
By: Munirat Dawodu, RN, RM. Datelinehealth Africa Volunteer and Freelance writer. Medically reviewed by: Tii Ngwachi Munghieng, M, and K Craig, MB BS. MPH.
A round global map in red colour, captioned: “Why sickle cell burden is high in Africa”. There is an oval picture of a young black family of three at the top pole of the globe representing the human nature of the condition.
Sickle Cell Disease (SCD) is not a new condition in Africa. We've known about it, lived with it, and lost loved ones to it for decades. Yet, instead of reducing, the numbers are rising in many communities across the continent.
So the question that keeps coming up is simple: If we talk so much about sickle cell, why do the numbers continue to rise?
Working in the clinics as a student nurse has shown me that the real problem is not just a lack of awareness. The problem is that awareness is often surface-level, fear-based, and often disconnected from the real decisions people face in relationships, homes, and communities. (4)
People have heard of sickle cell, but many still don't understand how it translates to illness, when to get tested, or why genetic considerations are important for their children’s health. (3)This gap in understanding continues to shape real-life decisions, relationships, pregnancies, and ultimately, health outcomes.
This article explains the human, cultural, and systemic factors behind sickle cell disease in Africa, using simple, evidence-based, and relatable language rooted in our lived reality.
.jpg)
An infographic summarising the burden of Sickle Cell Disease in Africa and globally. Data from WHO (2025)
The SCD statistics in Africa tell a story that should worry every public health system.
According to the World Health Organization, about 515,000 babies are born with SCD every year, and more than 75% of these births happen in sub-Saharan Africa. (5) Nigeria alone is estimated to contribute 30% of all global SCD births, making it one of the leading countries with the highest burden of sickle cell disorder in the world. (7)
In Nigeria, the high SCD birth numbers, despite decades of awareness indicate a gap between awareness and effective prevention. The high SCD trait prevalence (about 20–25%) means many families could be at risk, but without systematic screening, counselling, or preventive interventions, risk remains high.
In high-income countries with universal newborn screening and comprehensive SCD care, most children with SCD survive into adulthood. In many parts of sub-Saharan Africa, up to 50–90% of children with SCD die before their fifth birthday because of poor diagnosis and inadequate care. (6)
These numbers don’t only represent babies born with the disease, they expose a health system failure to:
In other words, the problem is the gap between what we know about SCD and what we do about it and this gap is costing lives.
“Biology, environmental factors, cultural choices, and gaps in health systems keep SCD numbers high.”
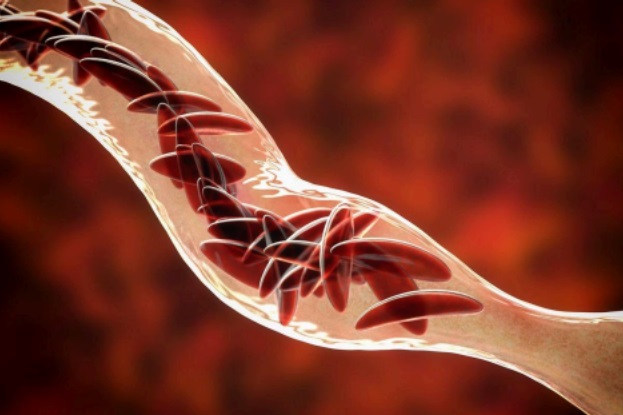
An illustration of a blood vessel with sickle red blood cells binding together to blcok the vessel. This is a key feature of Sickle Cell Disease. (SCD) Image Credit: National Institutes of Health
SCD remains common in Africa because:
With the increasing number of SCD in Africa, most people assume Africans do not yield to or follow genetics or medical counsel. But this idea could miss out on the real reasons: biology, cultural choices, and gaps in health systems that keep the numbers high.
Another reason why the sickle cell gene (HbSS) is very common in Sub-Saharan Africa is that people with the sickle cell trait or one sickle gene (HbAS) have some protection against severe malaria, so the trait is passed on more often. (1)
Due to this protective advantage, many of those with the trait don’t die from severe malaria and pass it down to their children and the cycle continues. But SCD only occurs when a child inherits the sickle gene from both parents (SS).
Although many people know about the trait, turning that knowledge into helpful decisions is the bigger problem. They may recognise labels like AA, AS, and SS, but not what they really mean for children and families. (3) Someone may know they are AS but not how it affects their choices about relationships or having children. A couple may understand the risk but hope they will be the exception. Families often make decisions based on hope, love, pressure, or religion long before medical risks enter the conversation. (4)
Another problem is that the genotype tests are sometimes unreliable or unavailable. In some areas, accurate tests are expensive while the cheaper ones sometimes give the wrong results. Some people rely on old or low-quality test results and may later find out that the results were incorrect.
Lack of routine newborn and early childhood screening means many children who carry the sickle-cell trait (AS) are never identified early. Without this information, families grow up unaware of their genetic risks. By the time these children reach adulthood, they begin relationships and plan families without knowing their genotype, increasing the chance of AS-AS pairings, and ultimately, more SCD births. (8)
“In many communities, SCD education is event-based, rather than continuous health education, which limits long-term understanding and behaviour change.”

Photo of a young African female health worker in brightly coloured dress with a big smile, speaking with two mothers carrying their babies about infant care in an outdoor clinic. AI generated image credit from Freepik
Community education about Sickle Cell Disease (SCD) in Africa is widespread, but the messages are often unclear or incomplete. (2) There are SCD awareness campaigns, posters, social media messages, and church seminars, but many of these efforts lack the depth needed to influence real decisions about genotype testing and prevention.
In many communities, SCD education is event-based, rather than continuous health education, which limits long-term understanding and behaviour change.
Communities only hear about sickle cell during an occasional school health talk, a yearly church seminar, or World Sickle Cell Day events with posters and radio jingles. After these brief events, the messages fade, leaving young couples and parents without the consistent guidance needed for real-life decisions like premarital genotype testing and childbearing.
Another major problem is that much of our SCD education is delivered in technical language that does not match the community’s health literacy levels or daily experiences, which weakens people’s understanding of how SCD is inherited or prevented.
A 2023 study among parents of children with SCD in Benin found that overall SCD knowledge was low. Only about 29% of parents scored 70% or higher on a disease knowledge questionnaire, even though they were connected to SCD care. (2) This finding shows that awareness or even regular contact with healthcare services does not automatically guarantee a clear or understandable SCD education.
.jpg)
A diagram illustrating the probability of inheritance of Sickle Cell Disease (SCD) when both parents carry the Sickle Cell Trait
In many African communities, decisions about marriage and childbearing are shaped by several factors such as expectations, tradition, faith, and the weight of communal norms. (4) When two young people find out they both carry the sickle cell trait (AS), deciding whether to marry or have children is rarely just personal: it becomes a crossroads of love, hope, faith, and uncertainty. Sometimes, couples make decisions without full disclosure or understanding.
There was once a sickle cell patient whose mother admitted that his father concealed his genotype so they could marry. Stories like this highlight how incomplete information, social pressure, and fear of stigma can override careful decision-making, and why genetic counselling, open and supportive communication are crucial for family health decisions.
In a 2025 study among parents of children living with sickle cell disease in Nigeria, only 14.5% of couples had mutual premarital genotype awareness before marriage, meaning both partners knew both their own and each other’s genotype before marriage. (4)
This low awareness isn’t necessarily about carelessness. Rather, it highlights that genetic awareness requires proper education, emotional preparedness, and social support. Without accessible premarital genetic counselling or community-level education, many couples make life-changing decisions based on incomplete understanding or social pressure.
“For a condition as common and life-impacting as sickle cell, prevention should be a national health priority, yet in many countries, individuals are left to figure it out.”
One major reason why SCD remains widespread in Africa is that prevention through screening, counselling, and early diagnosis is not fully operational in the national healthcare systems.
In many countries:
For a condition as common and life-impacting as sickle cell, prevention should be a national health priority, yet in many African countries, individuals are left to figure it out. As a result, many families make decisions not based on structured health guidance, but on emotion, social pressure, and hearsay.
“SCD persists in Africa because genetic information is not reaching people early enough, clearly enough, or consistently enough.”

A male African health worker with a friendly smile wearing a lab coat, speaking casually with a mother sitting in a community outdoor clinic and carrying her baby on her lap. This type of encounter is a good point for health workers to convey information to parents of newborn babies in African communities about early genetic screening for sickle cell disease. AI generated image from: Freepik
The statistics make one thing clear: SCD persists in Africa because genetic information is not reaching people early enough, clearly enough, or consistently enough.
With more than 20–25% of Nigerians carrying the AS genotype, and up to 80% of global SCD births happening in sub-Saharan Africa, community stakeholders have an essential role to play in bridging the gap between awareness and actual prevention.
These can be achieved through the following:
Most families only begin paying attention to genotype at the point of engagement or pregnancy, which is already late in the decision-making process.
If communities normalised genotype testing in secondary school, during youth group programs, premarital counselling in religious centres, and routine health fairs, people would make informed decisions years before emotions, pressure, and expectations complicate everything.
A recent study shows that many AS–AS couples do not separate because of emotional attachment, family expectations, religious pressure, belief that “God will intervene regardless of genotype”. (4) Communities can create safe spaces where:
In many African settings, community behaviour changes fastest when the message comes from religious leaders, elders, teachers, and local women groups, and youth mentors. These are the voices that shape decisions more than any poster or hospital lecture.
If these influencers speak clearly about genotype, counselling, and prevention, the message reaches deeper than technical health campaigns ever could.
Communities can organise:
When the AS prevalence is as high as 1 in 4 people, genetic literacy must become everyday knowledge not specialised knowledge.
Many families hide SCD diagnoses out of shame.
Communities can change this by:
Empathy encourages others to seek help early, which is critical because up to 50–90% of African children with SCD die before age 5 when support is missing. (6)
Preventing sickle cell disease does not require perfect systems, it requires practical, reproducible steps that communities, health systems, and individuals can actually implement. Based on current data and the gaps we see across Africa, these are the most effective prevention strategies:
Where available, professional counselling helps couples translate genotype knowledge into practical decisions.
Counselling can clarify risk percentages (for AS–AS couples, 25% chance of having a child with SCD) and discuss options such as family planning, IVF with genetic testing, or early prenatal diagnosis.
Routine health visits, immunisation days, or school health programs are opportunities to offer genotype testing and guidance.
Hospitals and clinics can bundle genotype testing with other services like malaria or anaemia screening, making it easier and less stigmatising to participate.
Families should document genotypes and SCD history across generations. Sharing this information with relatives, healthcare providers, and future partners ensures that decisions are informed, not based on assumptions.
In Africa, the impact of sickle cell disease is overwhelming. Daily, children living with the disease fight to stay alive, the parents burdened by uncertainty, and the families learning too late what they could have done differently. The numbers are staggering, but the real story lies in these human experiences.
What stands out most is this: prevention is possible through knowledge applied early, honest conversations, and social support from health workers, families, and communities. If we can make genotype testing routine, counselling accessible, and discussions about SCD normal, just like talking about blood type or allergies, lives can change.
Every small action matters. Every informed choice matters. And when communities, families, and the health system come together, the burden of SCD doesn’t have to be inevitable. We’ve known about SCD for decades, but now it’s time to translate knowledge into action. One informed family, one supported child, and one empowered community at a time.
Related:
How the Sickle Cell Trait Protects Against Malaria: A Simplified Scientific Explanation
Sickle Cell Disease: Essential Information for Africans
Published: December 21, 2025
© 2025. Datelinehealth Africa Inc. All rights reserved.
Permission is given to copy, use and share content for non-commercial purposes without alteration or modification and subject to source attribution.
DATELINEHEALTH AFRICA INC., is a digital publisher for informational and educational purposes and does not offer personal medical care and advice. If you have a medical problem needing routine or emergency attention, call your doctor or local emergency services immediately, or visit the nearest emergency room or the nearest hospital. You should consult your professional healthcare provider before starting any nutrition, diet, exercise, fitness, medical or wellness program mentioned or referenced in the DatelinehealthAfrica website. Click here for more disclaimer notice.


