Preeclampsia and Eclampsia: What Africans Need to Know
Author: Azuka Ezeike, MBBS, FWACS (Obstetrics and Gynaecology), FMCOG, MSc. (Public Health). Medically reviewed by the DLHA Team.
November 8, 2025
.jpg)
A pregnant Black woman wearing a blue maternity top sits in an examination room. Beside her are a digital blood pressure monitor, a stethoscope, and vials labelled “Magnesium Sulfate.” Image is AI generated with ChatGpt. Click to enlrge.
Whenever raised blood pressure (hypertension) is mentioned, your mind often may connect it with old age. So, for Mrs. Patience, the last thing on her mind when she got pregnant was hypertension. She was just 25 years old.
But in the seventh month of her pregnancy, during a routine antenatal visit, her blood pressure was found to be elevated. In addition, when her urine was checked, there was protein, which should not normally be present. This was how her journey with preeclampsia started. Preeclampsia is a condition that can endanger both mother and baby if not detected and treated early.
Info-poster captioned "Understanding Preeclampsia" and showing a pregnant tAfrican woman and a list of the features of the condition. Click on image to enlarge.
Preeclampsia is a disease of pregnancy characterised by elevated blood pressure (≥140/90 mm Hg) after the 5th month of pregnancy (20th week). It is associated with protein in the urine and damage to multiple organs in the body [1]. It can also occur after delivery, up to six weeks after delivery.
According to the International Society for the Study of Hypertension in Pregnancy (ISSHP), the diagnosis of preeclampsia can also be considered if there is elevated blood pressure with evidence of organ dysfunction, even if there is no protein in the urine
.jpg)
Table comparing the features of preeclampsia and eclampsia. Click on imge to enlarge.
Eclampsia is the onset of seizures (convulsions) or unexplained coma in a pregnant woman with preeclampsia in the absence of a neurological disease [2]. It is often considered a complication of preeclampsia. It can occur after the 20th week of pregnancy or even within six weeks after delivery. Sometimes, eclampsia can occur without preeclampsia manifesting first.
.jpg)
Infographics showing pregnancy related death rate attributed to preeclampsia in sub-Saharan Africa. Click on image to enlarge.
Preeclampsia affects 2 to 8% (i.e., 2 - 8 out of 100) pregnancies worldwide and results in the deaths of up to 46,000 women and 500,000 babies. In Asia and Africa, it accounts for up to 1 in 10 pregnancy-related deaths. In sub-Saharan Africa, hypertensive disorders are among the leading causes of pregnancy-associated deaths [3].
This article will help you understand what preeclampsia and eclampsia are, the factors that increase your risk, and how they can be detected early through antenatal care. You will also learn about the symptoms to watch out for, how doctors diagnose and manage the condition, and the steps you can take to protect yourself and your baby.
.jpg)
Risk factors of preeclampsia grouped into high and moderate. Click on image to enlarge.
Any pregnant woman can develop preeclampsia or eclampsia, but certain conditions increase the risk [1].
These risks are divided into two categories:
You are at high risk of developing hypertension in pregnancy if:
You are at moderate risk if:
Having these risk factors calls for vigilance. It doesn’t mean that preeclampsia or eclampsia must occur.
The exact cause of preeclampsia is not yet fully known [4]. This is why it was once known as the disease of theories. However, scientists are gaining a better understanding of the disease every day [5]. It is now believed the problem originates from the placenta.
In people predisposed to developing preeclampsia, blood flow to the placenta is reduced very early in pregnancy. The lack of adequate blood supply causes the placenta to produce certain chemicals (biomarkers).
These chemicals damage the lining (endothelium) of tiny blood vessels throughout the body; causing endothelial dysfunction. This explains why preeclampsia can affect multiple organs.
Endothelial dysfunction is believed to be the major cause of preeclampsia, although other factors may also contribute and are still being studied [1].
This damage causes leakage of protein and fluid from blood vessels into surrounding tissues, leading to swelling. When protein leaks from the blood vessels in the kidneys, it results in the presence of protein in the urine.
Preeclampsia is traditionally classified into two types:
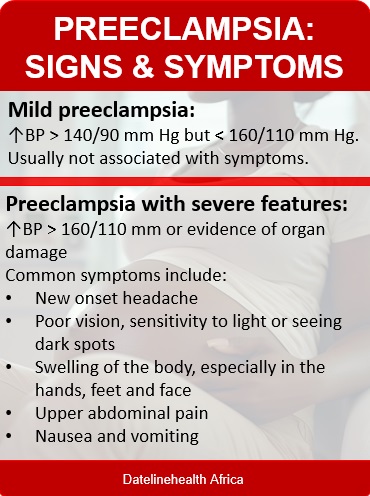
Info-poster showing signs and symptoms of preeclampsia. Click on image to enlarge.
The symptoms of preeclampsia may vary among patients, but the common ones include:
Eclampsia usually manifests as convulsions or, in some cases, sudden coma.
The presence of these symptoms indicates severity and the need for urgent delivery.
To determine if you have preeclampsia, your doctor will ask you some questions, examine you, and carry out a few tests.
This is in accordance with the recommendation of the ISSHP.
You are likely to be pregnant or have just delivered.
Your doctor will want to know:
Your doctor will:
These will include:
Because the problem that causes preeclampsia/eclampsia originates in the placenta, the best treatment is delivery.
This is usually done if the pregnancy is up to 34 weeks, which is the period when your baby’s lungs are expected to have matured (well-developed)
If the pregnancy is less than 34 weeks, your doctor may decide to admit you for observation, provided: [6]
During this period, you will be admitted to the hospital, and the following will be monitored:
You will also be given some medications, which may include:
You will also be advised to arrange for blood donation at the blood bank, as delivery may become urgent.
Your doctor will observe you in the hospital until your blood pressure returns to normal. In most cases, you may be monitored for up to 7 days, as blood pressure sometimes rises between days 3 and 6 after delivery.
After discharge, your doctor will schedule periodic follow-up appointments until 6 weeks after delivery.
Ensure you take your drugs as prescribed and follow all instructions from your doctor during this period.
Preeclampsia and eclampsia can affect several organs in the mother’s body and may also harm the baby [1]. Without proper medical care, both can become life-threatening.
These conditions can lead to serious complications, including:
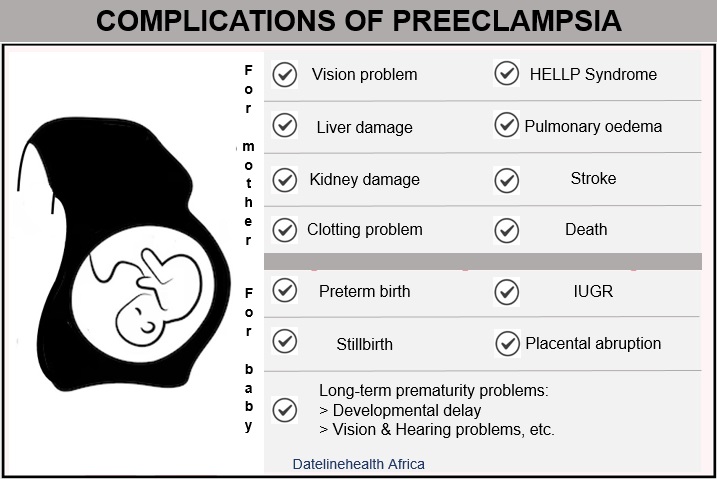
Info-poster: Complications of preeclampsia for mother and baby
When preeclampsia affects blood flow to the placenta, the baby may not get enough oxygen and nutrients. This can lead to:
If you are pregnant, contact your doctor immediately if you notice persistent headaches, unusual swelling of your hands or face, or blurred vision.
Preeclampsia and eclampsia remain major causes of illness and death among pregnant women, especially in Africa, but they are preventable and treatable when detected early. Regular antenatal visits, awareness of warning signs, and prompt medical attention can save lives. Every pregnant woman should take blood pressure checks seriously and seek help immediately if she notices symptoms such as severe headaches, swelling, or blurred vision. With proper care and timely delivery, both mother and baby can make a safe recovery.
1. Can preeclampsia be prevented?
Although the risk of preeclampsia cannot be eliminated, the World Health Organization (WHO) recommends the following measures for prevention:
2. Will preeclampsia affect future pregnancies?
Having preeclampsia does not automatically mean that future pregnancies will be affected. However, women who have had preeclampsia are at a higher risk of developing it again in subsequent pregnancies, especially if it occurred early or was severe. Regular antenatal care and early monitoring are essential in future pregnancies.
1. Karrar SA, Martingano DJ, Hong PL. Preeclampsia. [Updated 2024 Feb. 25]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 [Cited 2025 Oct 3]. Available from here.
2. Magley M, Hinson MR. Eclampsia. [Updated 2024 Oct. 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 [Cited 2025 Oct 3]. Available from here.
3. Musarandega R, Nyakura M, Machekano R, Pattinson R, Munjanja SP. Causes of maternal mortality in Sub-Saharan Africa: A systematic review of studies published from 2015 to 2020. J Glob Health. 2021;11:04048. doi: 10.7189/jogh.11.04048. Available from here.
4. Santulli G, Kansakar U, Varzideh F. Epidemiology and pathophysiology of preeclampsia: New mechanistic insights. Hypertension. 2025 May;82(5):800–3. doi: 10.1161/HYPERTENSIONAHA.124.24117. Available from here.
5. Erez O, Romero R, Jung E, Chaemsaithong P, Bosco M, Suksai M, et al. Preeclampsia/eclampsia: the conceptual evolution of a syndrome. Am J Obstet Gynecol. 2022 Feb;226(2 Suppl):S786–803. Available from here.
6. Sharma DD, Chandresh NR, Javed A, Girgis P, Zeeshan M, Fatima SS, et al. The management of preeclampsia: a comprehensive review of current practices and future directions. Cureus. 2024;16(1):e51512. Available from here.
Related:
Understanding Hypertension in Pregnancy
Social Factors Shaping African Women’s Health
What Africans need to know about Antenatal care
Published: November 8 , 2025
© 2025 Datelinehealth Africa Inc. All rights reserved.
Permission is given to copy, use, and share content freely for non-commercial purposes without alteration or modification and subject to source attribution.
DATELINEHEALTH AFRICA INC., is a digital publisher for informational and educational purposes and does not offer personal medical care and advice. If you have a medical problem needing routine or emergency attention, call your doctor or local emergency services immediately, or visit the nearest emergency room or the nearest hospital. You should consult your professional healthcare provider before starting any nutrition, diet, exercise, fitness, medical or wellness program mentioned or referenced in the DatelinehealthAfrica website. Click here for more disclaimer notice.
.jpg)


