Food Allergies and Intolerance in African Adults: Causes, Diagnosis and Prevention
By Victory Onyenekwe. B.Sc. Ed Physical and Health Education. Freelance Health Writer. Medically reviewed by The DLHA Team.
March 28, 2026

An African female patient receives oxygen by nasal mask for a severe allergic reaction, in a busy hospital emergency centre. Image credit: Google Gemini. Click on image to enlarge.
“Africans never have food allergies.” How many times have you heard this?
For most African adults, food allergies are often viewed as a foreign concept peculiar to our Western counterparts. Ingrained in our minds is the assumption that we cannot be allergic to our traditional meals. This belief is reinforced by a lack of data, as localized studies on food allergies are minimal, with many reported claims of “allergy” in African adults actually turn out to be food intolerances.
Distinguishing between the two is vital: one is a digestive inconvenience, while the other can be life-threatening leading to severe breathing and cardiovascular problems (anaphylaxis). Consequently, food allergies are not something that should be ignored.
In this article we examine the critical differences between food allergies and intolerance, how they are diagnosed and actionable prevention and management tailored to the African context.
A food allergy is a reaction to a food protein that occurs in the immune system. The body mistakenly considers this food protein as harmful, triggering a protective response. Food allergy responses can be categorized into the following:
IgE-Mediated Food Allergies: The IgE (Immunoglobulin E) is an antibody in the immune system that is triggered when the body is exposed to an allergen. An example of this category of allergy is the Pollen-Food Allergy Syndrome, a condition where an individual’s body is already sensitized to certain pollens such as grass. The body then confuses the proteins in raw vegetables and fruits for the pollen proteins it is allergic to. This syndrome often appears when eating raw fruit or salads; however, the cross-reactive proteins can be destroyed when cooked.
Symptoms of an IgE-mediated food allergy occur within seconds or minutes of consumption or exposure to an allergen.
Non- IgE Mediated Food Allergies: This allergic reaction occurs without involving the IgE antibody. Symptoms are delayed, typically developing between 2 to 72 hours. This makes them harder to identify through medical screening. Standard food allergy tests such as the skin-prick test and blood test usually return negative results in these cases because they only screen for IgE antibodies.
Mixed IgE and Non-IgE-mediated: This is a combination of both IgE and non-IgE reactions
Food intolerance is the inability of an individuals’ body to digest certain food substances found in particular meals. Generally resulting in bloating, flatulence (farting) or diarrhoea. This is usually caused by an enzyme deficiency, sensitivity to food additives, or a reaction to naturally occurring chemicals. Food intolerance takes place in the digestive system.
.jpg)
Infographics showing burden of food allergies in Africa relative to all allergic reactions. Click on image to enlarge.
While localised research is limited, available studies suggest that food allergies account for anywhere from 5% to nearly 50% of all allergic reactions across the continent. [1]
Emerging evidence indicates that food allergy is becoming a significant health concern in Africa, mirroring trends previously seen in Western nations. In South Africa, 42% of children with atopic dermatitis were confirmed to have a food allergy through oral food challenges, with peanut allergy rates within this group reaching 26%.
The data also highlights a gap between perception and clinical reality. While self-reported allergy rates in some regions are as high as 17-19%, clinical testing in parts of Ghana and Nigeria reveals a lower true prevalence of 3-5%. Furthermore, the African allergenic landscapes are distinguished from Western patterns by regional allergens like pineapple, okra and mopane worm.[2]
Ultimately, a lack of clinical resources and limited access to testing facilities in many countries continue to hinder the collection of comprehensive data.
While Africans can be allergic to common global allergens, there are regional allergens that differentiate the African allergenic landscape from its Western counterparts, largely due to variations in local diets and regional environments.
The top 9 global allergens are:
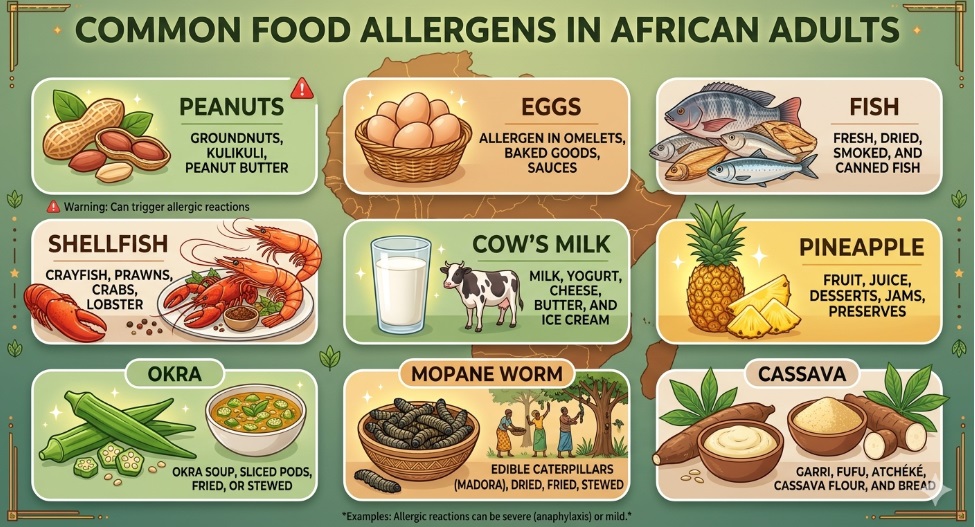
Info poster showing the common food allergens in African adults. Image credit: Google Gemini. Click on image to enlarge.
Here is a list of the common foods in Africa that people are usually allergic to:
Related: Allergies on the Rise in Africa
Food intolerance across the African continent is most commonly linked to lactose (dairy). But the use of traditional fermented products often breaks down lactose and makes it easier to digest.
Other intolerances can arise from fructose in high-sugar fruits and honey, as well as gluten. Often, these intolerances go unrecorded because many individuals primarily consume indigenous staples, meaning they may not be frequently exposed to high fructose and gluten-containing foods enough to realize they have a sensitivity to them.
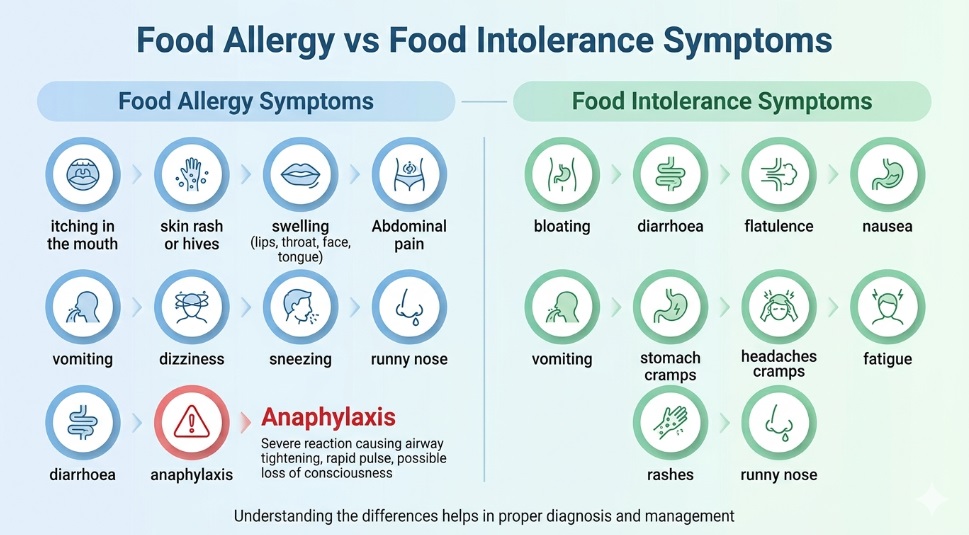
Info poster displaying the symptoms of food allergies and intolerance. Image credit: Google Gemini. Click on image to enlarge.
Food allergy symptoms typically occur within minutes and may involve the skin, gastrointestinal tract, respiratory system, and cardiovascular system. The following are common symptoms of food allergies:
Some common symptoms of food intolerance include:
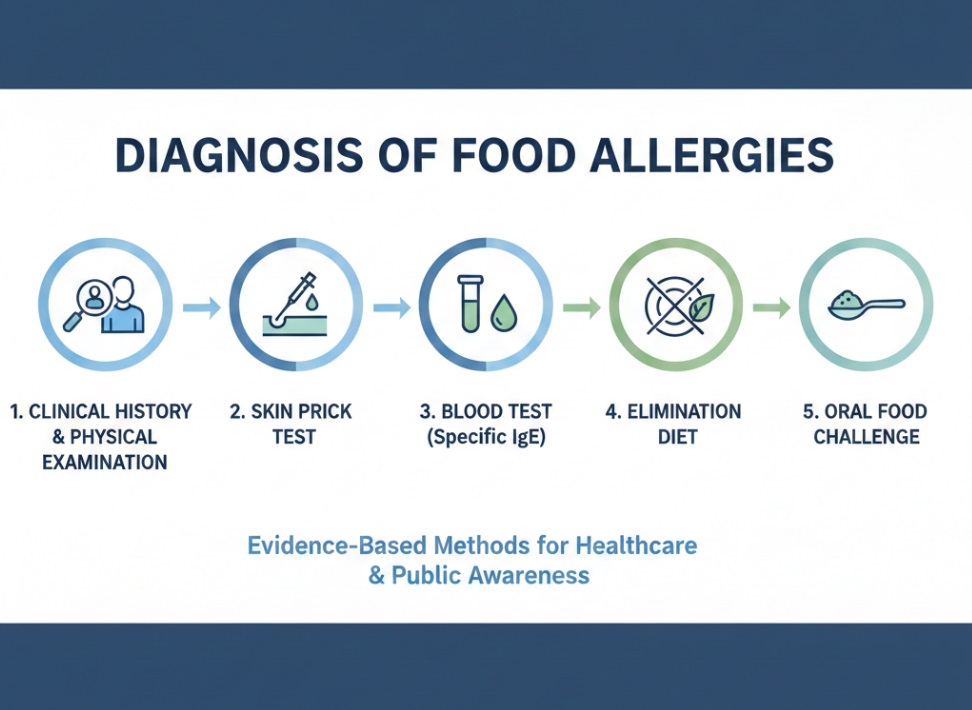
Info poster showing steps in the diagnosis of food allergies. Image credit: Google Gemini. Click on image to enlarge.
Diagnosis of food allergy in Africa, remains challenging. In many settings, adequate facilities for food allergy testing are lacking. Additionally, allergic reactions are often overlooked especially when they are not life-threatening.
Here are the steps involved in the diagnosis of food allergies
I. Clinical History and Physical Exam: A doctor will conduct a comprehensive medical review, which includes evaluating:
II. Allergy Testing: An allergy test can be carried out in two ways:
It is important to note that a positive skin prick test does not always indicate a true allergy. If a patient is scheduled for this test, and is currently taking antihistamines, the medication should be stopped two- five days before the test will be carried out, to ensure accurate results.
Unlike skin test, the blood test is not affected by antihistamines. However, they show sensitisation rather than certainty as blood tests can yield false positive results.
III. Elimination Diet: This involves removing specific foods suspected of triggering an allergic reaction. Symptoms are closely monitored, followed by a supervised reintroduction of the suspected food to the patient. This process should only be done under medical guidance.
IV. Oral Food Challenge (OFC): Considered the most accurate form of diagnosis of food allergy. OFC involves giving a patient an increasing amounts of a suspected allergen to confirm or rule out an allergy. This must only be conducted under strict medical supervision.
Related: Eczema in African Adults: Causes, Types and Symptoms
Food allergy testing is not without its faults or flaws. Here are some common mistakes in food allergy testing:
Effective management of food allergies in African adults should focus on preventing exposure, identifying reactions promptly, treating symptoms, and public awareness.
Related: Asthma in African Children: Causes, Symptoms and Care
It is critical to recognize that Africans are not immune to food allergies. There is a profound need for increased investment in well-designed, appropriate studies to generate accurate data and reliable evidence specifically for this demographic.
This evidence will support the development of effective health policies and targeted interventions, ensuring that Africans have access to proper diagnosis, specialized treatment, and long-term care for food allergies.
Additionally, raising public awareness and strengthening local healthcare infrastructure are essential steps toward reducing misconceptions and improving clinical outcomes for affected adults. By prioritizing education for both the public and healthcare providers, we can reduce the risk of misdiagnosis and ensure that people do not cut out important traditional foods without a medical reason.
No, Men and women do not develop food allergies equally. At childhood and adolescence boys are more likely to be affected by food allergies than girls. However, as women get older, they become more likely to be affected by food allergies due to hormonal influences with oestrogen producing a stronger immune response. This higher prevalence normalizes or decreases as menopause sets in.
Yes, you can develop an allergy to food consumed for years. This new reaction can be triggered by environmental changes, or a prolonged break from eating a specific food.
No, food intolerance is not the same as food poisoning. Food intolerance is your body’s inability to digest certain substances found in your food, leading to bloating, flatulence and diarrhoea while food poisoning is an acute illness that is caused by the consumption of food that has been contaminated by bacteria, viruses or toxins generally resulting in fever and vomiting.
1. Mvoundza Ndjindji O, Djoba Siawaya JF. Mapping Allergic Diseases in Sub-Saharan Africa. Front Allergy. 2022; 3:850291. Doi:10.3389/falgy.2022.850291. Available from here.
2. Kung SJ, Steenhoff AP, Gray C. Food allergy in Africa: myth or reality? Clin Rev Allergy Immunol. 2014 Jun;46(3):241-9. doi: 10.1007/s12016-012-8341-z. (Abstract). Available from here.
3. Fleischer D, Burks A. Pitfalls in Food Allergy Testing Diagnosis: Serum IgE Testing. The Journal of Pediatrics. 2014;166.8-10. (Editorial). Available from here.
Published: March 28, 2026
© 2026. Dateline Health Africa Inc. All rights reserved.
Permission is given to copy, use and share content for non-commercial purpose without alteration or modification and subject to source attribution.
DATELINEHEALTH AFRICA INC., is a digital publisher for informational and educational purposes and does not offer personal medical care and advice. If you have a medical problem needing routine or emergency attention, call your doctor or local emergency services immediately, or visit the nearest emergency room or the nearest hospital. You should consult your professional healthcare provider before starting any nutrition, diet, exercise, fitness, medical or wellness program mentioned or referenced in the DatelinehealthAfrica website. Click here for more disclaimer notice.


