Haemorrhoids: What Africans Need to Know
By: Elizabeth Obigwe, B.Sc. Anatomy. Freelance Health Writer. Medically reviewed by: A. Odutola, MBBS, PhD, FRCSEd
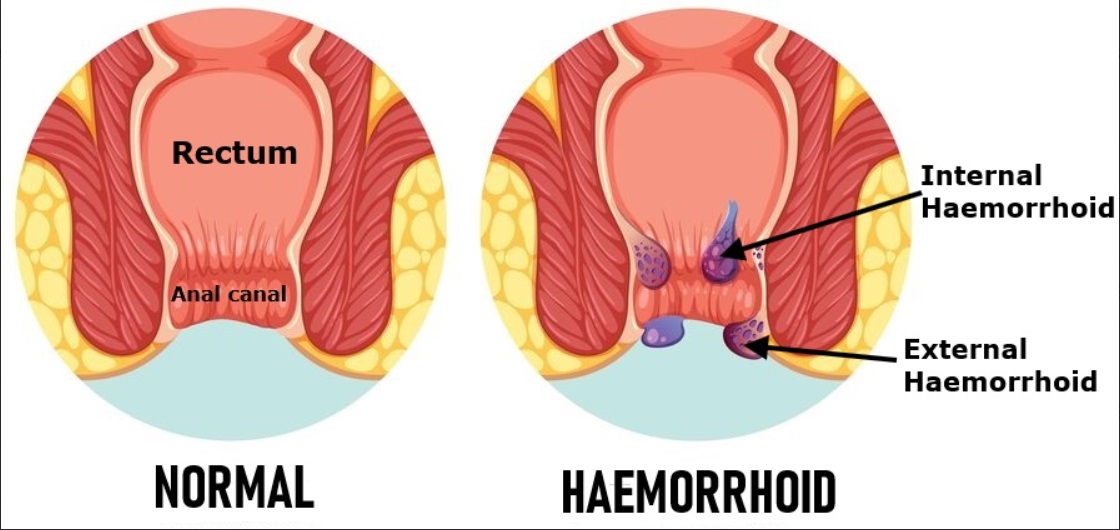
Illustration comparing normal anorectal anatomy with that in haemorrhoids. Image credit: Freepik
Have you ever heard someone say that they have piles, “jedi-jedi”, or “kooko”? These are some of the common names Africans use to describe haemorrhoids. Some scientists also describe it as “varicose veins of the anus and rectum.”
Haemorrhoids affect the anal canal (back body) and can make passing stool uncomfortable or difficult. Not every anal problem is caused by haemorrhoids.
This article will explain haemorrhoids in detail to help Africans identify and understand the condition. The article will cover the following:
Haemorrhoids are swollen blood vessels (veins) around the exterior of the anus (back body) or inside the lower part of the rectum (last part of the large intestine just above the anus) that can cause discomfort, bleeding, or itching.
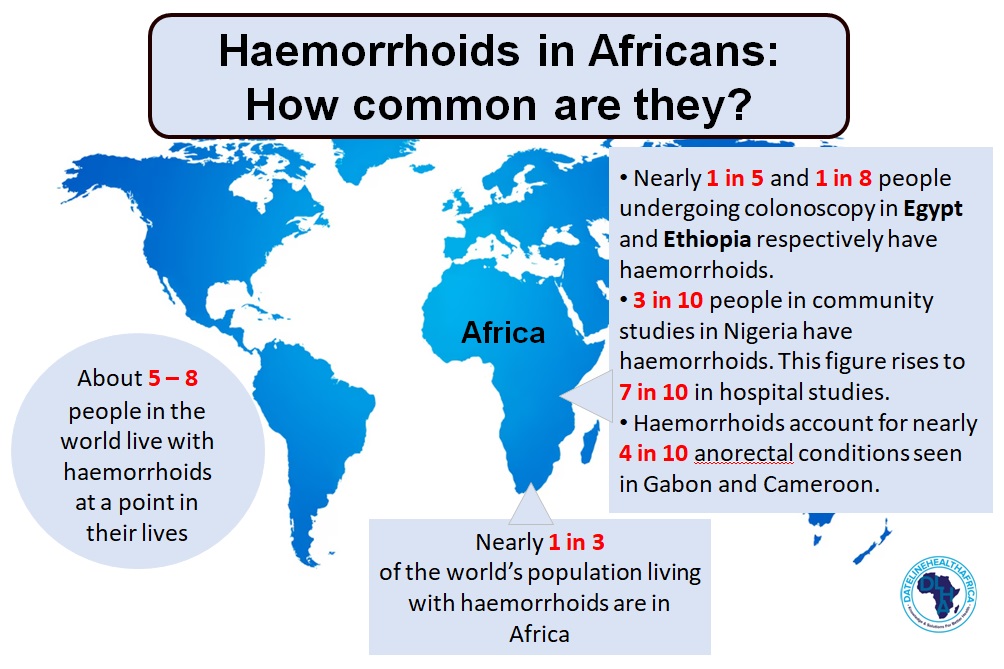
Fig. 1: Infograpics showing the rates of occurence of haemorrhoids globally nd in different African countries.
Haemorrhoids are quite common in people within and outside of Africa. It is estimated that 50 to 85% of the world’s population will be affected by haemorrhoids at some time in their lives [1].
One systematic review found that of all the people in the world living with haemorrhoids at a given time, nearly 1 in 3 (28%) were from Africa. However, the prevalence of the condition varies widely across African countries (see fig. 1).
For example, haemorrhoids have been reported in nearly 1 in 5 (18%) and 1 in 8 (13%) of adults patients in Egypt and Ethiopia respectively who undergo colonoscopy, a procedure performed to check the health status of the large bowel.
In Nigeria report of community occurrence of haemorrhoids is as low as 1 in 33 (3.3%) people. But much higher rate of occurrence has been reported in Nigerian hospital settings, where they account for up to 7 in 10 (72.3%) of anorectal (terminal bowel) clinic cases.
In Central Africa (Gabon) and Cameroon, haemorrhoids make up nearly 4 in 10 (38.5%) and 40.83% respectively of anorectal diseases [2].
Although it can occur at any age, this condition is more common among adults 20-50 years of age [1]. Also, the condition affects both men and women at almost the same rate.
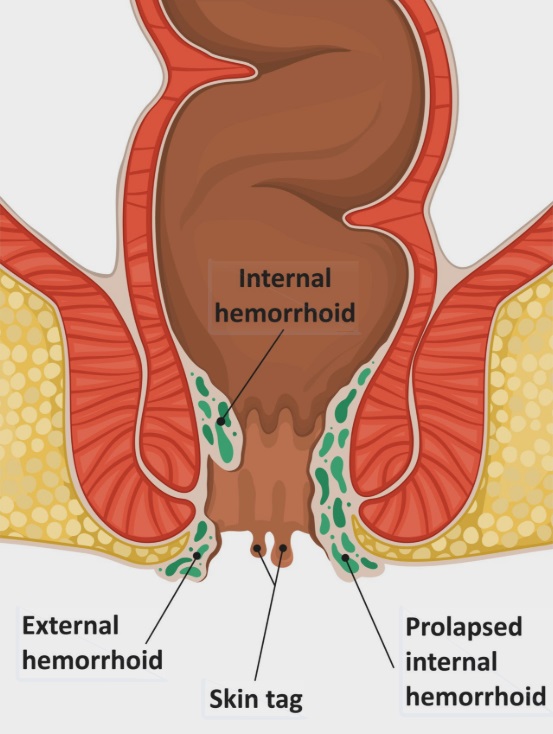
Fig. 2: Cartoon illustration of the anorectal region showing internal haemorrhoids inside the anal canal and external haemorrhoids around the anus. Gemini AI generated image.
Haemorrhoids are grouped into internal and external types based on where they are located [3] (See fig. 2).
External haemorrhoids are found outside the anus. Because they have pain-sensing nerves, they are usually painful, especially when swollen or inflamed.
Internal haemorrhoids are found inside the anus. They usually do not cause pain because they lack pain-sensing nerves, but they may bleed or prolapse (bulge out of the anus).
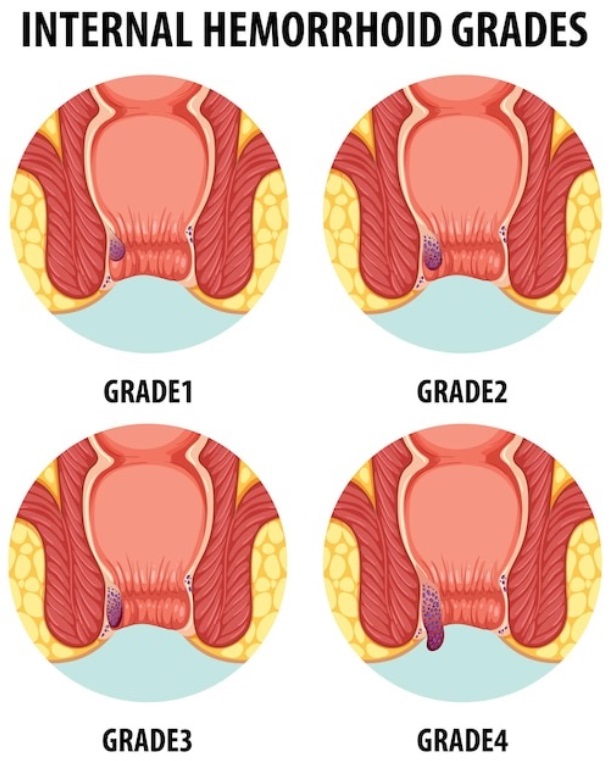
Fig. 3: Cartoon illustration showing the four grades of internal haemorrhoids, from grade one through to grade four with permanently prolapsed haemorrhoids.
Internal haemorrhoids can further be graded based on how much they come out of the anus [3]. See fig. 3):

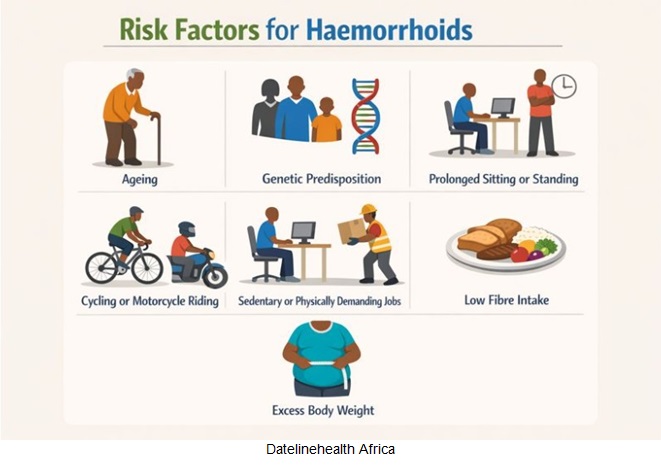
Info poster showing some of the common causes of haemorrhoids
Haemorrhoids happen when the blood vessels (veins) around the anus are under too much pressure for too long, or blood doesn’t flow out of them as it should. This can cause the veins to stretch, bulge, and may become inflamed or bleed. Some factors that can increase pressure on the vein or affect blood flow are [4, 5];
Other factors that generally increase your chances of developing haemorrhoids include [4, 5];
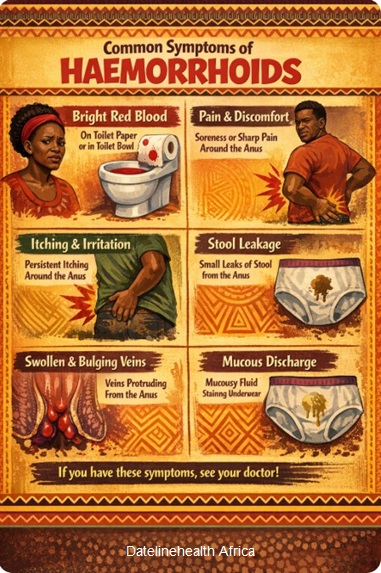
Info poster showing some of the common symptoms of haemorrhoids
Some symptoms that have been associated with haemorrhoids include [6];
Note that some of these symptoms are not limited to haemorrhoids, but may also be seen in other conditions that affect the rectum and anus. For example, bleeding from the anus can also be associated with colon cancer and inflammatory bowel diseases. Hence, you should seek medical attention for proper diagnosis and confirmation.
It is advisable to see a doctor when symptoms are severe, persistent, or unusual. See a doctor if:
Some people are quick to attribute any pain, bleeding, or discomfort around the anus to haemorrhoids, but this is not always true. That is why proper diagnosis is important to make sure the symptoms are truly caused by haemorrhoids and not another condition.
To diagnose you of haemorrhoids, your doctor starts by taking your medical and family history. He will also ask about the symptoms you are experiencing.
During the physical examination, the doctor may examine your abdomen, then your anal area, while you are relaxed and sometimes while straining. This helps reveal external haemorrhoids or internal haemorrhoids that have prolapsed.
A gentle finger examination of the rectum may also be done to check for lumps, pain, or infection. But internal haemorrhoids are often not felt unless they are large or prolapsed.
If needed, a short instrument called an anoscope may be used to look inside the anus. This allows the doctor to see internal haemorrhoids directly, which often appear as swollen, purplish bulges.
In some cases, especially when there is ongoing bleeding or increased risk of cancer, your doctor may recommend tests such as a colonoscopy to examine the colon more fully and rule out other possible diseases [7].
Depending on severity, haemorrhoids may resolve by themselves or following certain home remedies. In more severe cases, it may require a minimally invasive procedure or even surgery.
Eating more fibre (fruits, vegetables, whole grains) helps soften stools and reduces straining. There are lots of fibre-rich foods in Africa. You can also take fibre supplements if necessary, but you should talk to your healthcare provider first.
Staying hydrated helps keep stools soft.
This helps to reduce pressure on anal veins.
Sitting in warm water several times a day eases pain and swelling.
Products with witch hazel, lidocaine, or hydrocortisone can relieve pain and itching.
Simple pain medicines like acetaminophen or ibuprofen can reduce discomfort [8]
II. Medical procedures
A doctor places a small rubber band around the base of an internal haemorrhoid to cut off its blood supply so it shrinks and falls off.
A solution is injected into the haemorrhoid to shrink it.
Heat from infrared light is used to shrink the haemorrhoid.
Surgical removal of large or severely prolapsed haemorrhoids. It is done under anaesthesia.
A stapling device is used to reposition internal haemorrhoidal tissue and reduce prolapse.
A minimally invasive procedure where the blood vessels feeding the haemorrhoids are tied off to shrink them [7, 9].
There are many myths/misconceptions about haemorrhoids across Africa. Table 1 illustrates some of these beliefs and the medical facts that clarify them [10,11]. It is important to debunk these wrong beliefs because they often promote unnecessary shame or fear in people and delay the seeking of professional medical help.
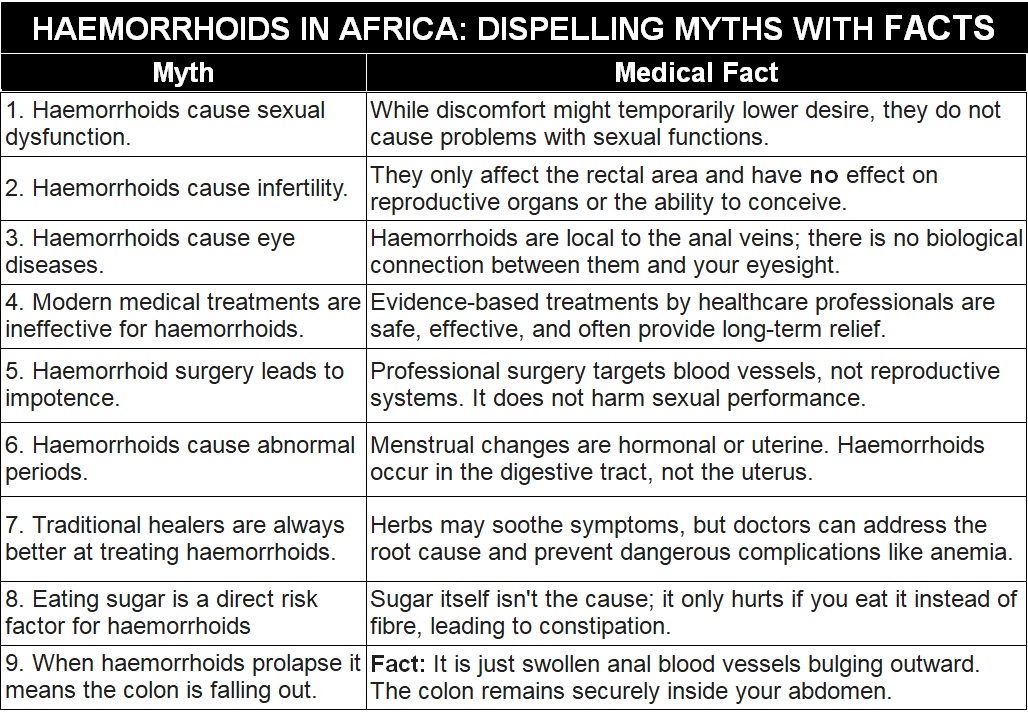
Table 1: Shows some of myths/misconception about hemorrhoids that are common among Africans and the medical facts that debunk them.
Understanding that haemorrhoids are a localized vascular issue helps in choosing the right path for treatment—which usually involves increasing fibre, hydration, and seeking professional medical advice.
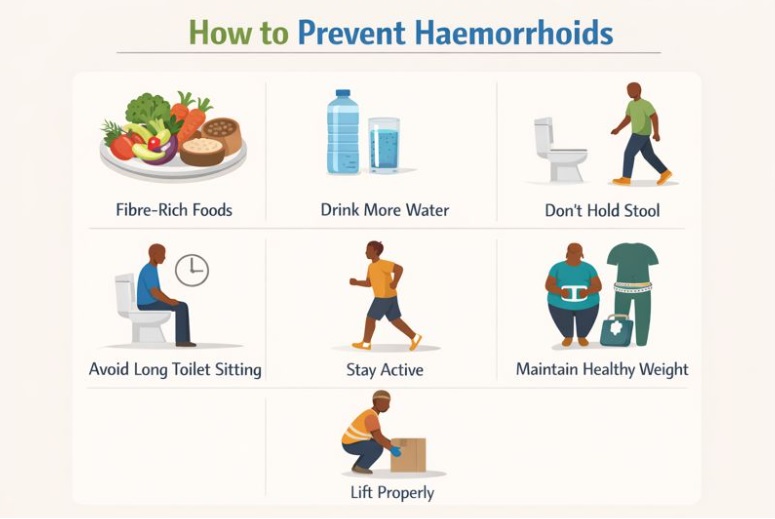
Info poster showing some hemorrhoid prevention tips.
Some of the things you can do to prevent haemorrhoids from occurring are;
Haemorrhoids are a common condition, but they are often misunderstood or surrounded by silence. In many parts of Africa, misinformation and shame cause people to delay care, rely on unsafe remedies, or live with unnecessary pain. Haemorrhoids are a manageable health condition that responds well to simple lifestyle changes and timely medical care. Early action prevents complications, reduces the need for surgery, and protects quality of life.
1. Omale MK, Adegboye OO. A ten-year study of the management of hemorrhoids at a secondary nursing home in South-West Nigeria. Int Res J Pharm. 2012;3:198–200. Available from here.
2. Esmaeilnia Shirvani A, Pakdaman K, Maleki Z, Soraneh S, Rezaei Chegini F, Pakdaman K, Vali M, Nikbakht HA, Shojaie L, Ebrahimi P. Worldwide prevalence of haemorrhoids: a systematic review and meta-analysis. Ann Med. 2026;58(1):2606433. doi:10.1080/07853890.2025.2606433. Available from here.
3. Ray-Offor E, Amadi S. Hemorrhoidal disease: predilection sites, pattern of presentation, and treatment. Ann Afr Med. 2019;18(1):12–16. doi:10.4103/aam.aam_4_18. Available from here.
4. Nassa YG, Danjuma A, Ayuba SB, Yahaya SA, Inusa B, Yakubu I. Prevalence and predictors of hemorrhoids among commercial motorcyclists in Kaduna State, Nigeria. World J Prev Med. 2016;4(1):1–4. Available from here.
5. Kibret AA, Oumer M, Moges AM. Prevalence and associated factors of hemorrhoids among adult patients visiting the surgical outpatient department at the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia. PLoS One. 2021;16(4):e0249736. doi:10.1371/journal.pone.0249736. Available from here.
6. Sandler RS, Peery AF. Rethinking what we know about hemorrhoids. Clin Gastroenterol Hepatol. 2018. doi:10.1016/j.cgh.2018.03.020. Available from here.
7. Mott T, Latimer K, Edwards C. Hemorrhoids: diagnosis and treatment options. Am Fam Physician. 2018;97(3):172–179. Available from here.
8. National Institute of Diabetes and Digestive and Kidney Diseases. Treatment of hemorrhoids [Internet]. U.S. Department of Health and Human Services; [Last reviewed Oct. 2016}. Cited 2026 Jan 20. Available from here.
9. Hawkins AT, Davis BR, Bhama AR, Fang SH, Dawes AJ, Feingold DL, et al. The American Society of Colon and Rectal Surgeons clinical practice guidelines for the management of hemorrhoids. Dis Colon Rectum. 2024;67(5):614–623. doi:10.1097/DCR.0000000000003276. Available from here.
10. Azeez A, Isiugo-Abanihe UC. Sociocultural context and determinants of treatments for hemorrhoids among the Nigerian police, Oyo State command. J Soc Behav Health Sci. 2017;11(1):3. Available from here.
11. Mahassadi AK, Motcheyo HC, Kouame DH, Yao-Bathaix FM. The perception and practices of Black African subjects toward hemorrhoidal disease: effects of beliefs and misconceptions in Côte d’Ivoire, West Africa. Res Rep Trop Med. 2025;16:11–23. doi:10.2147/RRTM.S498009. Available from here.
Related: Inflammatory bowel disease simplified for Africans
Published: February 5, 2026
© 2026. Datelinehealth Africa Inc. All rights reserved.
Permission is given to copy, use and share content freely for non-commercial purposes without alteration or modification and subject to attribution as to source.
DATELINEHEALTH AFRICA INC., is a digital publisher for informational and educational purposes and does not offer personal medical care and advice. If you have a medical problem needing routine or emergency attention, call your doctor or local emergency services immediately, or visit the nearest emergency room or the nearest hospital. You should consult your professional healthcare provider before starting any nutrition, diet, exercise, fitness, medical or wellness program mentioned or referenced in the DatelinehealthAfrica website. Click here for more disclaimer notice.


