GERD Explained to Africans: Symptoms and Treatment
By Oluwasola Samuel, Freelance Health Writer. Medically reviewed by A. Odutola. MB BS, PhD, FRCSEd.
An AI-generated image of an African man wearing a light grey T-shirt, sitting and holding his chest in apparent pain .
Click on image to enarge.
Introduction
Do you often feel a burning pain in your chest after a meal or a heavy dinner? Many Africans shrug it off, but when it keeps happening, it could be more than just spicy food. It might be GERD, a condition where stomach acid repeatedly flows back into the throat, causing discomfort and sometimes serious complications.
In recent years, GERD has quietly become more common across Africa. Many people still confuse GERD with an ulcer, a heart condition, or indigestion. This delays proper diagnosis and treatment.
In this article, you will learn about GERD from these viewpoints:
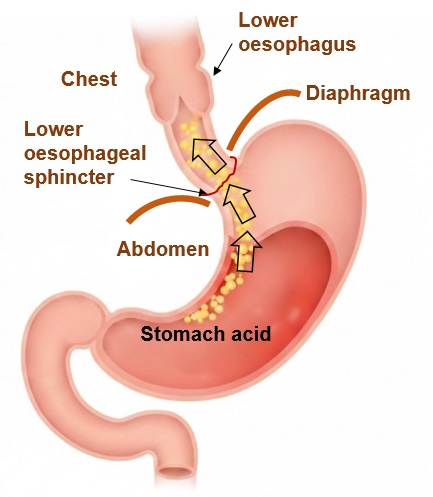
Fig. 1: Illustration showing how GERD occurs through reflux of stomach acid into the lower oesophagus due to weakness in the lower oesophageal sphincter (LOS). Click on image to enlarge.
GERD, also known as gastroesophageal reflux disease, is a common cause for patient visits to their doctors. When severe, it can affect the quality of life of patients and cause emotional, social, and physical dysfunctions, as well as work related concerns.
GERD happens when stomach acid repeatedly flows backwards into your oesophagus (the narrow tube or food pipe that connects your mouth to your stomach). See fig. 1. Normally, there is a small muscle at the bottom of your oesophagus called the lower oesophageal sphincter (LOS). It is like a one-way valve that opens to let food pass into your stomach, then closes tightly to keep acid where it belongs, in the stomach.
But when this valve (LOS) becomes weak or relaxes too often, acid from your stomach escapes upward. That is when you feel the burning sensation in your chest or throat, often called heartburn.
Over time, this acid can cause inflammation, throat irritation, or even make swallowing painful (dysphagia). If untreated, GERD can damage the lining of your oesophagus and increase the risk of more serious complications. GERD means acid reflux happens frequently (at least twice a week or more). At this stage, it becomes a health concern and needs immediate medical attention.
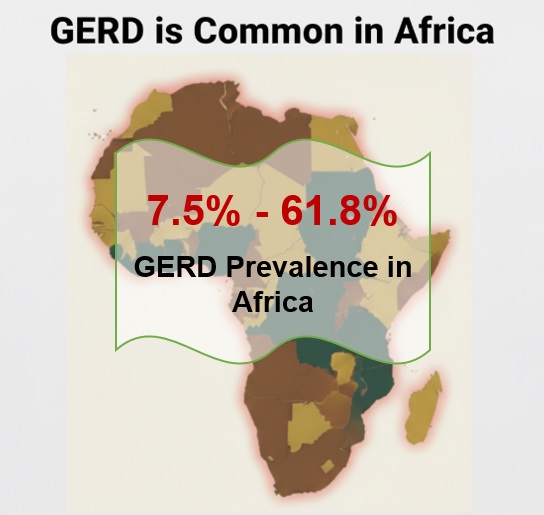
Fig.2: Infographic showing an unlabeled map of African countries with an overlay of data on the wide range of GERD prevalence across Africa. Click on image to enlarge.
.
Gastroesophageal reflux disease (GERD) affects many Africans, but the real numbers are still unclear. (See Fig. 2).
There is limited research across the continent, so we don’t fully know how widespread it is. However, a major study in Nigeria found that approximately 7.6% of adults in the country experience GERD symptoms [1]. Interestingly, the study also found that GERD often overlaps with other digestive issues like indigestion and irritable bowel syndrome (IBS), suggesting the problem may be more complex than we think.
In South Africa, a study reported a prevalence of 22.9% in women and 4.1% in men, showing that gender may play a role in who gets affected [2]. Meanwhile, a broader review of multiple regional studies identified GERD prevalence rates across Africa to be in the range of 7.6% to 61.8%, depending on which community is studied and the diagnostic method used [3].
Even though GERD may not be as common in Africa as in some Western countries, the trend shows it’s becoming more of a public health concern.
Despite these findings, large-scale studies on GERD in Africa are still limited. This means many people living with GERD might go undiagnosed or untreated. Researchers agree that more studies are needed to understand how GERD truly affects Africans.
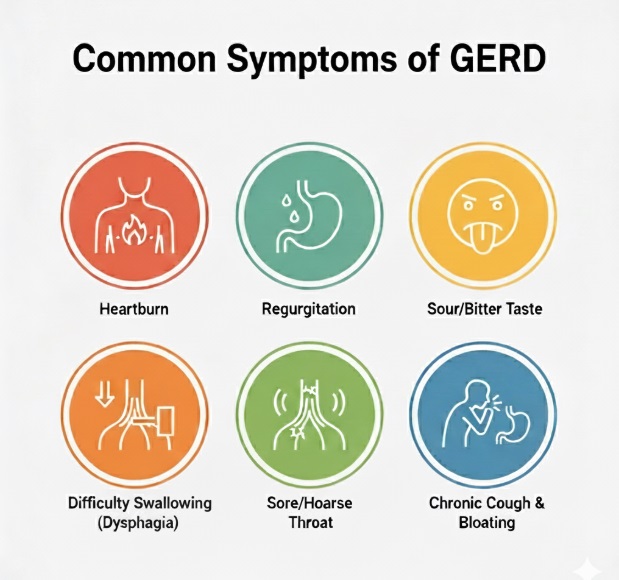
Fig. 3: Info poster showing some of the symptoms of GERD (Gastroesophageal reflux disease); feelings of burning in the chest, regurgitation, sour taste in the mouth, trouble swallowing, sore throat, and frequent cough. Click on image to enlarge
GERD doesn’t always affect everyone the same way, but there are some symptoms that you may have that suggest acid flowing back up your oesophagus.
Some of the symptoms include (see Fig. 3).
This is the most noticeable sign. You begin to experience a burning pain in your chest, usually after eating. It may feel worse when you bend over or lie down, especially after a heavy or spicy meal.
When stomach acid moves upward, it can leave a sour or bitter taste. Sometimes, it makes your throat feel raw. You might even wake up at night with this unpleasant taste in your mouth.
GERD can make swallowing painful or give the sensation that food is stuck in your throat. This happens when the acid irritates and inflames (swells) your oesophagus.
The stomach acid can irritate your throat and vocal cords, leading to a hoarse voice or chronic cough. If you have a cough that just won’t go away, especially one that gets worse at night, it could be caused by GERD.
Some people with GERD often feel bloated, nauseous, or uncomfortable after eating, as if the food just won’t settle. This is common when you eat too fast or have large portions, something that often happens at social gatherings or in late dinners.
6. Chest Pain that Feels Like Heart Trouble
GERD-related chest pain can be similar to heart problems. It’s important to pay attention if you experience shortness of breath, dizziness, or pain around your arm or jaw. Kindly see a doctor immediately to rule out heart issues.
Many people mistake GERD for an ulcer or gas trouble. While they can share similar symptoms, ulcers are caused by sores in the stomach lining, whereas GERD is about acid moving the wrong way.
GERD is caused by a weakness in the lower oesophageal sphincter (LOS) that allows stomach acid to reflux into the lower oesophagus (food pipe). The exact causes of the weakness of the LOS are not fully known, but may include a hiatal hernia and other risk factors discussed below. A hiatal hernia is a push of part of the stomach through an opening in the diaphragm into the lower chest. The diaphragm is a muscle that is used in breathing and separates the chest from the abdomen.
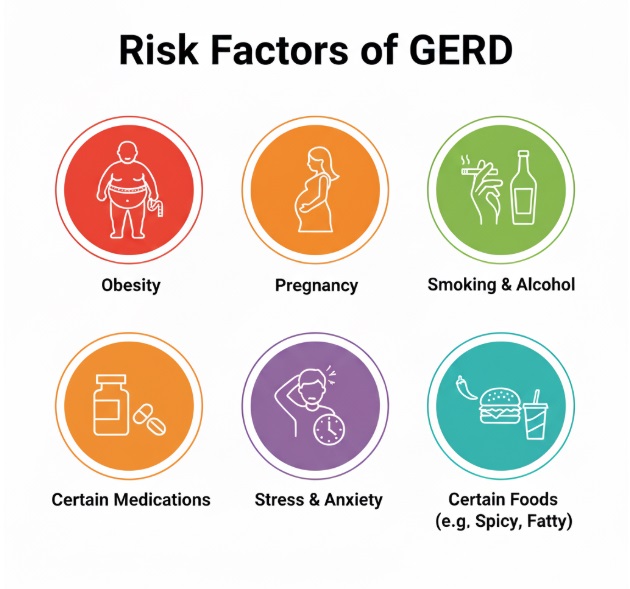
Fig 4 Info poster showing some of the symptoms of GERD (Gastroesophageal reflux disease): obesity, pregnancy, smoking and alcohol, certain medications, stress, and certain types of food. Click on image to enlarge.
There are several factors that increase your risk of GERD. It is important to note them and avoid them to lower your risk.
These risk factors include (see Fig. 4):
Eating a heavy or spicy meal, especially at night, is a risk factor. In many African homes, dinner is often the heaviest meal of the day, with rich soups, fried foods, or spicy stews eaten at that time of day. After such meals, most people lie down almost immediately, which allows acid to flow into the oesophagus.
Fried and oily food like Nigerian “puff-puff” (fried dough balls), “akara” (fried bean cake), “suya” (spicy beef jerky), fried plantain, and oily stews can relax the lower oesophageal sphincter (LOS). When this happens, acid slips upward, leading to heartburn.
Alcohol relaxes the LOS muscle, while smoking reduces saliva production. Together, they increase your chances of acid reflux. Sadly, both habits are common among young African adults, especially during social events or stressful periods [4].
Extra weight, especially around the belly, puts pressure on your stomach and pushes acid upward into the throat. With increasing rates of obesity in Africa’s urban regions, more people are unknowingly putting themselves at risk of GERD.
During pregnancy, hormonal changes relax body muscles, including the LOS. The growing baby also presses on the stomach, making acid reflux more likely. Heartburn is very common in pregnant African women, especially in the third trimester [5].
Some medications, such as painkillers, asthma drugs, or muscle relaxants, can worsen reflux. In many African settings, the frequent use of herbal bitters or traditional tonics for digestion may also irritate the stomach lining and worsen over-the-counter drugs.
Stress doesn’t cause GERD directly, but it can worsen symptoms. Many people undergo stress in their daily lives. Many skip meals during the day and overeat at night, especially after work. This irregular eating pattern increases acid buildup and reflux.
In many African countries, healthcare access varies widely. Some people have access to modern diagnostic facilities, while others, especially those living in rural areas do not.
Here are some of the ways GERD can be diagnosed:
Clinical diagnosis is often the first step. Here, your healthcare professional (HCP) will listen to your complaints, ask several questions about your symptoms, including its duration, diet and feeding habits, alcohol use, medications taken, etc. Your HCP will then check your body physically, with special attention to your abdomen and chest.
If you are experiencing heartburn twice a week or more, along with other typical symptoms and physical findings in support, your HCP may diagnose GERD based on their clinical assessment before ordering further tests as they may consider necessary.
The diagnostic tests may include:
This is the gold standard test when available. A catheter (a thin, flexible tube with a camera) is passed down your throat to examine your oesophagus and stomach. This lets your HCP see any damage, inflammation, or complications.
This test measures acid levels in your oesophagus over 24 hours. A small probe is placed through your nose into your oesophagus. The other end outside is connected to a recording device that's attached to your belt or a strap around your waist.
Here, the sensor at the tip of the catheter, carefully guided into your oesophagus, measures acidity levels and transmits data to the recorder.
This involves the use of an X-ray to check for abnormalities in your oesophagus. This involves drinking a chalky liquid that shows up on X-rays. As it goes down, X-rays are taken to look for abnormalities. This is more widely available than endoscopy in many African settings.
This test checks how well your oesophagus moves food down into your stomach. It checks how strong the muscles in your oesophagus are and how they contract. It also checks how the LOS opens and closes.
This test helps your HCP understand where the problem might be and how to find a lasting treatment.
This test is done to look for any damage in the oesophagus. A catheter is put through your nose and moved down your throat into your oesophagus. The camera sends pictures to a video screen. This allows your HCP to have a live visual of what's happening inside of you.
The good news about GERD is that it can be treated. In many cases, simple lifestyle changes can make a big difference. However, if symptoms are frequent or severe, your HCP may recommend medication or, in rare cases, surgery.
Here are some of the treatment options:
Lifestyle changes are some of the ways to help manage and treat GERD. If these lifestyle changes are practised, they can significantly help manage this condition. This type of treatment involves voluntary changes that improve quality of life.
Some of the lifestyle changes that helps with GERD are:
If lifestyle changes do not improve your symptoms, your healthcare provider may ask you to start taking medications that may include:
Antacids neutralise stomach acid and provide quick relief. They work within minutes but only last 30 minutes to an hour. They are good for occasional heartburn but not for regular use. Side effects can include diarrhoea (magnesium-based) or constipation (calcium- or aluminium-based).
These blockers reduce acid production. Examples include famotidine and cimetidine. They work within an hour and last longer than antacids, usually 6 to 12 hours. They are good for mild to moderate GERD. You can take them before meals to prevent symptoms.
Low-dose PPIs are available over the counter. Examples include omeprazole, lansoprazole, and esomeprazole. These are the most effective medications for reducing acid. It takes them 30 to 60 minutes before your first meal of the day. They take a few days to reach full effectiveness but provide 24-hour relief once they do.
When lifestyle changes and medication do not give the desired results, you might be advised to consider surgery to help improve your symptoms and quality of life. A detailed consideration of the surgery types is beyond the scope of this article.
The outcome of treatment of GERD is generally good. You are likely to see early symptom relief with changes in diet, lifestyle and medication use (PPIs). Long term relief often requires ongoing care and relapse of symptoms is common when treatment is stopped. In some people, especially those who do not receive adequate care, complications may occur.
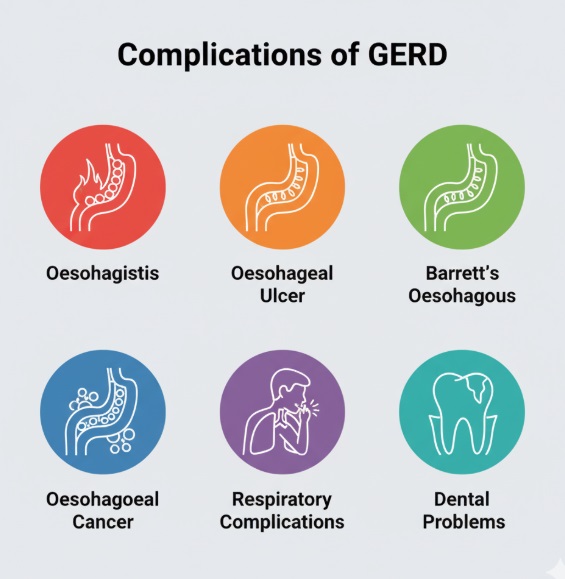
Fig 5 Info poster showing some complications of GERD (Gastroesophageal reflux disease): oesophagitis, oesophageal ulcer, Barrett's oesophagus, oesophageal cancer, respiratory complications, and dental problems. Click on image to enlarge.
Chronic and untreated GERD can lead to unpleasant complications that can be life-threatening.
Below are some of the complications that can arise when GERD is chronic or left untreated:
1. Chronic oesophagitis (inflammation of the oesophagus)
When stomach acid repeatedly refluxes into your oesophagus, it damages the delicate lining. The stomach has a thick mucus layer and special cells that protect it from acid. Your oesophagus doesn't have these protections. As a result, repeated acid exposure causes inflammation, redness, and swelling of the oesophageal lining.
2. Oesophageal stricture (narrowing of the oesophagus)
When oesophagitis persists for months or years, the chronic inflammation triggers a healing response (repair damaged tissues) [6]. Scar tissue forms in the oesophageal lining. Unlike normal oesophageal tissue, which is flexible, scar tissue is rigid and doesn't stretch. As scar tissue builds up, it causes the oesophagus to narrow.
3. Barrett's oesophagus
Normally, your oesophagus is lined with flat, thin cells called squamous cells. (6) When these cells are repeatedly exposed to stomach acid, some of them change. They transform into different cells. This transformation is your body's attempt to protect itself. So your oesophagus tries to adapt by replacing its normal cells with more acid-resistant cells. These new cells sometimes are abnormal and in the wrong place. As a result, they pose a small but real risk of becoming cancerous over time.
This is the most feared complication of GERD, though it's important to note that most people with GERD may never develop oesophageal cancer. Why oesophageal cancer is so serious is that it is often caught late because early-stage oesophageal cancer usually doesn't cause symptoms. By the time symptoms appear (difficulty swallowing, weight loss, chest pain), the cancer has often spread.
When acid touches your throat and voice box, it triggers a cough reflex. Chronic cough is one of the most common respiratory complications. This cough is usually dry (no mucus). The cough can be severe and persistent, lasting for months or years. It disrupts sleep, interferes with work, and is socially embarrassing.
Your teeth aren't designed for acid exposure. The enamel protecting your teeth is remarkably strong but can dissolve when exposed to acid. When stomach acid reaches your mouth, whether through vomiting or silent reflux, it erodes tooth enamel.
Dental erosion from GERD typically affects the back surfaces of your front teeth and the chewing surfaces of your back teeth. The erosion leads to several dental problems, like being sensitive to hot, cold, or sweet foods and drinks.
Just like your stomach can develop ulcers, so can your oesophagus. Oesophageal ulcers can be extremely painful. Swallowing becomes difficult and painful. You might avoid eating because it hurts so much, leading to weight loss. The ulcers can sometimes bleed severely.
Feeling frequent burning chest pain that won't stop is common when it's GERD. However, knowing when to just grab some antacids and when to call your doctor can make a huge difference.
If you experience any of the following, consider reaching out to your doctor:
GERD is more than just heartburn. It's a chronic form of acid reflux that can seriously damage your oesophagus if left untreated. But you have control over many of the risk factors. GERD is manageable with the right lifestyle changes and medical care when needed. Start with one change at a time. Small changes like losing weight, avoiding trigger foods, and quitting smoking can make a huge difference.
If you are experiencing symptoms more than twice a week, see a doctor before complications develop. Your health is in your hands. Better health outcomes start with the decisions you make today.
GERD is not a life-threatening condition and doesn't shorten your lifespan. People live completely normal lives with GERD, often for decades. It is a chronic condition you can manage and not something that determines how long you will live.
Acid reflux and GERD are related, but they are not exactly the same thing. Acid reflux is what happens when stomach acid flows back up into your oesophagus. It causes a burning sensation in your chest or throat, and honestly, almost everyone experiences it occasionally.
GERD (gastroesophageal reflux disease) is when acid reflux becomes chronic and frequent. If you are getting acid reflux more than twice a week, or it is severe enough to interfere with your daily life, that's when doctors call it GERD.
Yes, GERD can seriously disrupt your sleep. When you lie down, gravity stops helping keep stomach acid down, so it flows back up more easily. This causes heartburn, chest pain, coughing, or that bitter taste in your mouth that can wake you up multiple times or make it hard to fall asleep. Many people don't even realise their poor sleep is caused by GERD. Studies show people with nighttime GERD report worse sleep quality and more daytime sleepiness.
No, GERD itself does not cause death. It's a manageable chronic condition that affects millions of people. It sure can affect quality of life, but it doesn't directly cause death. With proper treatment like medications, lifestyle changes or surgery, most people control their symptoms well and live completely normal, full lives.
The only time GERD becomes life-threatening is when it is completely left unmanaged for many years. This can lead to grave life-threatening developments.
1. Nwokediuko SC, Adekanle O, Akere A, Olokoba A, Anyanechi C, Umar SM, et al. Gastroesophageal reflux disease in a typical African population: a symptom-based multicenter study. BMC Gastroenterol. 2020 Apr 15;20(1):107. Available from here.
2. Hunter MP, Crowther NJ. The prevalence of gastroesophageal reflux disease in an adult, South African black population, and the association with obesity. Minerva Gastroenterol Dietol. 2019 June;65(2):100–6. Available from here.
3. Al-Marhabi A, Hashem A, Zuberi BF, Onyekwere C, Lodhi I, Mounir M, et al. The views of African and Middle Eastern Gastroenterologists on the management of mild-to-moderate, non-erosive gastro-esophageal reflux disease (Gerd). Expert Review of Gastroenterology & Hepatology [Internet]. 2022 Mar 4;16(3):217–33. Available from here.
4. Oyewole BK, Animasahun VJ, Chapman HJ. Tobacco use in Nigerian youth: A systematic review. PLoS One. 2018 May 3;13(5):e0196362. Available from here.
5. Zhou S, Wang Y, Hou N, Hu K, Jiang S, You J, et al. Burden of gastroesophageal reflux disease among women of childbearing age, with projections to 2050: an analysis of the Global Burden of Disease study 2021. Front Glob Womens Health [Internet]. [cited 2025 Nov 9];6:1673878. Available from here.
6. Azer SA, Goosenberg E. Gastroesophageal Reflux Disease (GERD) [Updated 2025 Jul 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. [Cited 2025 Nov 9]. Available from here.
7. Chait MM. Gastroesophageal reflux disease: Important considerations for the older patients. World J Gastrointest Endosc [Internet]. 2010 Dec 16 [cited 2025 Nov 9];2(12):388–96. Available from here.
Related: Heartburn and Acid Reflux Explained to Africans: Symptoms and Treatment
Published: December 15, 2025
© 2025. Datelinehealth Africa Inc. All rights reserved.
Permission is given to copy, use, and share content freely for non-commercial purposes without alteration or modification and subject to source attribution.
DATELINEHEALTH AFRICA INC., is a digital publisher for informational and educational purposes and does not offer personal medical care and advice. If you have a medical problem needing routine or emergency attention, call your doctor or local emergency services immediately, or visit the nearest emergency room or the nearest hospital. You should consult your professional healthcare provider before starting any nutrition, diet, exercise, fitness, medical or wellness program mentioned or referenced in the DatelinehealthAfrica website. Click here for more disclaimer notice.


