Inflammatory Bowel Disease Simplified for Africans
By: Elizabeth Obigwe, B.Sc. Anatomy. Freelance Health Writer. Medically reviewed by A. Odutola, MB.BS, PhD, FRCSEd.
.jpg)
An illustration explaining inflammatory bowel disease and showing the internal wall of a normal colon, a colon with ulcerative colitis and a colon with Crohn's disease. Image credit: Freepik. Click on image to enlarge.
Almost everyone has experienced those uncomfortable, frequent trips to the restroom that seem to come out of nowhere. If you have had to make such unpleasant trips to pass watery stool three or more times in a day, it’s called diarrhoea. Most times, it’s caused by eating bad food or a mild infection and usually clears up after a few days, either on its own or with simple self-care measures, including over-the-counter medication.
However, diarrhoea isn’t always that harmless.
Sometimes, it’s a sign of something more serious than just an upset stomach. When diarrhoea keeps coming back or is accompanied by blood, abdominal pain, fatigue, or sudden weight loss, it may signal a more serious condition. These could be signs of Inflammatory Bowel Disease (IBD), a chronic condition that can affect daily life.
This article explains in simple terms all you need to know about Inflammatory Bowel Disease..
Inflammatory Bowel Disease (IBD) refers to a group of chronic disorders that cause inflammation in the digestive tract. It occurs when the body’s immune system mistakenly attacks the digestive tract, leading to long-term inflammation that damages the gut lining and disrupts normal digestion. Diseases like this, which are caused by the immune system's dysfunction, are called autoimmune disorders.
Inflammatory bowel diseases lead to periods of flare-ups (sudden burst of inflammation) and remission (improvement). They affect how the gut works and how well nutrients are absorbed. A flare-up occurs when the disease is active with increased inflammation and symptoms. In contrast, remission is the period of reduced inflammation and symptoms, even though the disease is still present.
There are two main types of inflammatory bowel diseases:
Each inflammatory bowel disease type is differentiated based on where in the digestive system (food channel) it occurs and how deeply it affects the intestinal wall. [1].
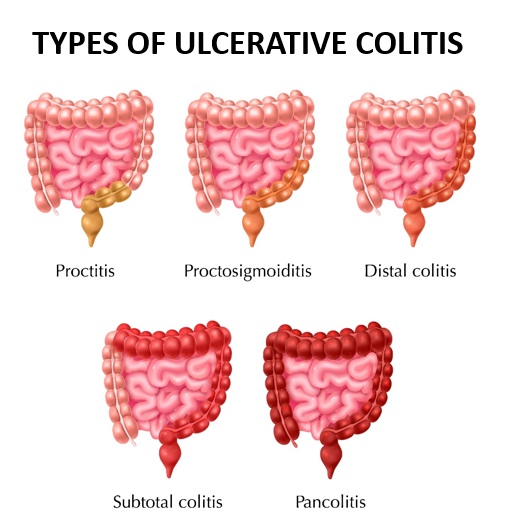
Fig. 1: An illustration showing how the intestine is affected by the different types of ulcerative colitis. Click on image to enlarge.
This involves inflammation of the inner lining of the colon (the longest part of the large intestine). It typically occurs in a continuous stretch, without skipping areas. Depending on the affected area, ulcerative colitis can be sub-grouped into: (See fig. 1)
2. Crohn's Disease (CD)
.jpg)
Fig 2: An illustration showing how Crohn's disease affects the colon. Click on image to enlarge.
Unlike ulcerative colitis, which affects only the inner mucosa lining, Crohn’s disease causes deep sores (called ulcers) that affect the entire thickness of the wall of the digestive tract. It can appear anywhere along the digestive tract, from the mouth to the anus.
However, it most commonly affects the lower small intestine (ileum) and the colon. The pattern of the disease is discontinuous. That is, it shows up in patches. You might have a damaged area followed by a healthy one, then another damaged area. (See fig. 2)
Crohn’s disease can appear in three main forms:
Other types of inflammatory bowel disease are indeterminate colitis (IC) and unclassified colitis (IBD-U) (other non-infectious inflammations of the bowel) [2].
.jpg)
Fig. 3: An illustration describing Irritable bowel syndrome and how it affects the colon.
Although IBD and IBS sound alike and share some symptoms, they are actually quite different conditions, and it is important not to confuse the two.
IBD stands for Inflammatory Bowel Disease and involves continuous inflammation and damage to the digestive tract. IBS, on the other hand, means Irritable Bowel Syndrome, a functional problem where the intestines appear normal but don’t work as they should. (See fig. 3)
While IBS doesn’t cause inflammation, bleeding, or visible injury as IBD does, it can still lead to discomfort such as stomach pain, bloating, diarrhoea, and constipation. However, IBS is generally less serious than IBD.
Fig. 4: Info poster: Global estimate of Inflammatory Bowel Disease as of 2019. Click on image to enlarge.
The exact number of people living with inflammatory bowel disease in Africa is still unclear because there has not been enough research on it, and so, the data is limited.
Misdiagnosis and underreporting of cases also make it difficult to know the true burden of the disease.
Interestingly, South Africa has always paid closer attention to IBD than many other sub-Saharan countries, and even when IBD was believed to be rare across the continent, South Africa continued to record significant cases [3]. This is likely because it is one of the region’s high-income countries.
Inflammatory bowel disease has long been viewed as a condition that primarily affects high-income countries, and while its prevalence remains higher in these countries, developing regions like sub-Saharan Africa, Asia, and Latin America have seen a clear rise in cases. This upward trend has contributed to a global increase.
Between 1990 and 2017, global incidence rose by 83.8%, while prevalence in sub-Saharan Africa increased by 31.5% in the West, 33.2% in the East, and 25.8% in the Central region [3].
By 2019, the Global Burden of Disease (GBD) estimated that about 5 million people worldwide were affected by IBD [2]. (See fig. 4)
Several factors have been linked to the rise in inflammatory bowel disease across Africa, including industrialisation and the adoption of more westernised lifestyles such as greater intake of processed foods and red meat, and lower fibre consumption [4]. Improved access to diagnostic facilities has also enabled health practitioners to make more accurate diagnoses [4].
Among the two main types of IBD, studies from Uganda, Kenya, Ghana, and Zimbabwe show that ulcerative colitis appears to be more common in sub-Saharan Africa than Crohn’s disease [3].
Earlier, we explained that IBD happens when the immune system mistakenly attacks the digestive tract. However, what triggers this misdirected attack is still not fully understood.
Scientists have proposed several ideas over the years, but there is no single, widely accepted cause of inflammatory bowel disease. What most experts do agree on, however, is that a mix of genetic and environmental factors likely plays role.
Scientists have observed that the following things (factors) that can increase people's chances of developing IBDs:
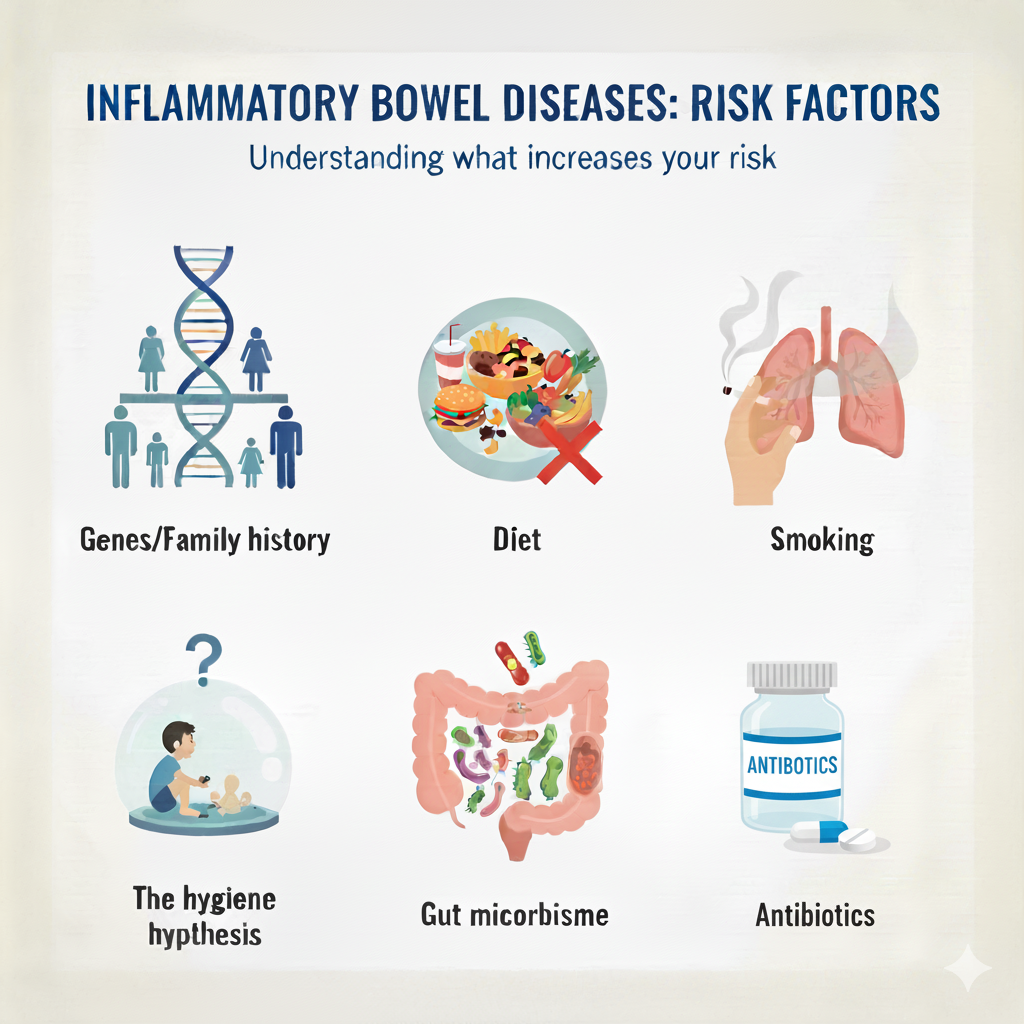
Fig. 5: Cartoon illustration, IBD risk factors. AI generated from Gemini. Click on image to enlarge.
1. Genes/Family history
Some people have genes that make them more likely to develop IBD. This gene is more common among white Americans than among Africans [3]. As a result, inflammatory bowel disease is higher among the former. Similarly, if you have a close relative who has suffered or is suffering from IBD, you have a higher chance of developing the disease than someone with no family history of IBD [5].
Because inflammatory bowel disease affects the digestive tract, what you eat or don't eat can play a major role. As more and more Africans adopt the Western lifestyle, including their diet, which is mostly processed foods, the risk of IBD in the region increases. The traditional African diet typically consists of vegetables, fruits, staple starches rich in fibre, and more. Consuming more of these tends to reduce the risk of developing IBDs [3].
Smoking has been linked with IBD, particularly Crohn's disease. A study in South Africa [3] found that 74% of patients with Crohn’s disease were smokers during the 6 months before diagnosis, or at the time of diagnosis.
This hypothesis states that if a child grows up in an overly sanitised environment, it can negatively affect the development of their immune system, making them susceptible to immune-driven diseases like IBD later in life. Sub-Saharan Africa has a high burden of infectious diseases and poor sanitation, which may be the reason for fewer cases of IBD in this region [3].
Reduction in the number as well as a change in the nature of the microorganisms found in the digestive tract has been linked to IBD. This alteration may be a result of dietary changes (eating more processed food), smoking, etc. [3].
Increased intake of antibiotics in both developed and developing countries is another factor that has been associated with high chances of developing IBD, especially Crohn's disease [2].
The symptoms of Crohn's disease and ulcerative colitis are similar and mostly involve the digestive tract, but they can also involve other parts of the body.
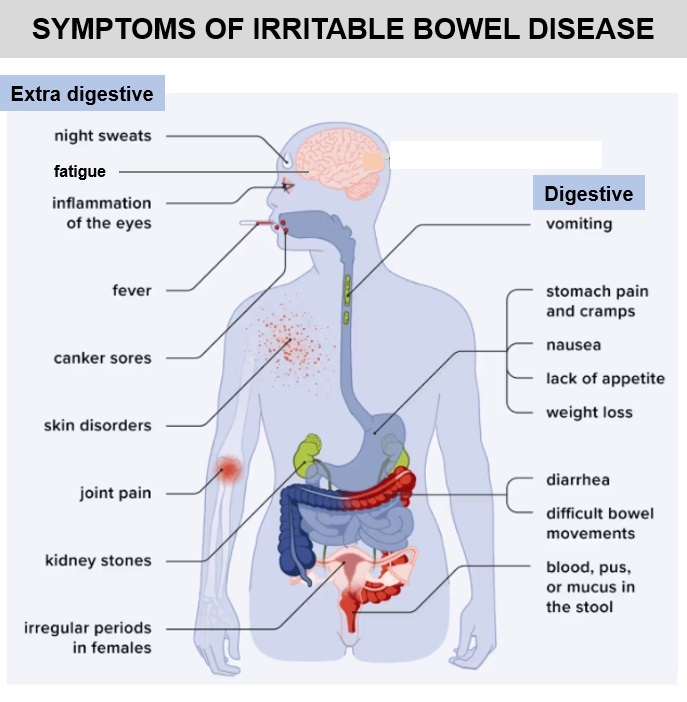
Cartoon illustration of the symptoms of IBD
See a doctor if you notice symptoms like frequent diarrhoea, severe abdominal pain, blood in stool, unexpected weight loss, or persistent fatigue or if these symptoms worsen. It is also important to seek medical help if new symptoms appear, medications stop working, or side effects occur. Generally, regular check-ups are key, even during remission, to monitor the condition and prevent complications.
Diagnosing inflammatory bowel disease usually involves several steps because its symptoms can look like those of other digestive problems. Your doctor combines information from your medical history, lab tests, scans, and a close look inside your digestive tract to confirm the diagnosis and rule out other possible causes.
Your doctor will start by having a detailed talk with you. They will ask about your symptoms, such as diarrhoea, abdominal pain, or weight loss and when they started. You’ll also be asked about your medical history, family history (since IBD can run in families), diet, lifestyle, and any medications you use.
Afterwards, the doctor will perform a physical examination to check for signs such as abdominal tenderness, weight changes, or symptoms outside the intestines, like joint pain or skin rashes. These help the doctor understand your overall health and decide which tests to order next [6].
Lab tests help detect signs of inflammation or complications. Some common lab tests include:
Endoscopy allows doctors to see inside the digestive tract using a flexible tube with a camera.
The most important test here is a colonoscopy, where the doctor looks inside the colon and rectum for inflammation, ulcers, or bleeding. During this test, small tissue samples (biopsies) are taken to confirm the diagnosis under a microscope.
If symptoms suggest upper digestive tract involvement (like in Crohn’s disease), the doctor may also perform an esophagogastroduodenoscopy (EGD), a test that examines the oesophagus, stomach, and upper small intestine [6].
Imaging helps doctors see parts of the digestive system that are difficult to reach with an endoscope and check for complications. It is like taking pictures of the digestive system beyond what the tube can show. Below are some of these tests [1, 6]
The treatment of inflammatory bowel diseases involves:
These are anti-inflammatory drugs that help calm down flare-ups quickly. They work by reducing the inflammation in your intestines and easing symptoms like pain, diarrhoea, and bleeding. However, they are not for long-term use because they can cause side effects like diabetes mellitus, eye problems, opportunistic infections, or weaker bones [7]. Doctors usually use them for short periods to bring IBD under control before switching to safer maintenance medicines.
These drugs help control an overactive immune system, which is the root cause of inflammatory bowel disease. They “train” your immune system to stop attacking your intestines. They take longer to work, but they’re useful for keeping the disease quiet after steroids have calmed a flare. Examples include:
Because they lower immunity, regular blood tests are needed to watch for side effects [7].
3. Biological Drugs (Biologics)
Biologics are modern, targeted medicines made from living cells. They block specific substances in your body that cause inflammation. They’re often used when other drugs don’t work well. Examples include:
Biologics are usually given through injections or infusions in hospitals [7].
These are newer, pill-based treatments that work inside immune cells to stop inflammation. They act faster than older immunosuppressants and are easier to take because they come as tablets, not injections.
Examples include: [7]
5. Aminosalicylates (5-ASAs)
These are among the oldest and safest drugs for ulcerative colitis (though less useful in Crohn’s disease). They help reduce inflammation directly in the lining of the bowel and are often used for mild to moderate UC.
Common examples are mesalamine and sulfasalazine.
They can be taken as pills or enemas, depending on which part of the colon is affected [7].
Diet can work alongside medications to improve how patients feel and recover. Recent findings [8] show that diet plays a powerful role in managing inflammatory bowel disease. What you eat can influence how much inflammation happens in your gut, how well your intestinal lining heals, and the balance between good and harmful bacteria in your digestive system. This is why following an informed inflammatory bowel disease diet can be an important part of treatment.
While liquid diets have traditionally been used to control symptoms, especially in children with Crohn’s disease, research now suggests that carefully planned whole-food diets can also help reduce flare-ups and support remission.
Living with inflammatory bowel disease can be challenging because it often comes with unpredictable flare-ups of symptoms like abdominal pain, diarrhoea, and fatigue, which can disrupt daily life, affecting the overall quality of life. Many people also experience emotional stress and worry about food choices. As such, medical care should not be limited to treating the physical symptoms only. It should take a holistic approach and also include psychological well-being [6].
Your doctor can suggest surgery when medications no longer work or serious complications arise. For ulcerative colitis, surgery may be needed if there’s severe bleeding, a hole in the intestine, or signs of cancer. It can also be considered when medicines fail to control symptoms or cause serious side effects that lower the quality of life [7].
For Crohn’s disease, surgery is usually recommended for patients whose disease does not respond to treatment, keeps coming back, or affects a specific part of the intestine, like the ileum and colon. However, surgery doesn’t cure Crohn’s disease. Symptoms often return after some time. Regular checkups with an endoscope help detect recurrence early and guide further care [7].
Diagnosing and treating inflammatory bowel diseases in Africa can be challenging for both the patient and the healthcare provider. Below are some of these challenges [3, 4].
Just like with the symptoms, complications due to IBD can affect the intestine or other parts of the body outside the intestine (intestinal or extra-intestinal complications) [1, 6].
Inflammatory Bowel Diseases arise when the immune system misfires and harms the digestive tract, leading to symptoms that can affect everyday life. While IBD used to be considered rare in Africa, we now know it is becoming more common. This is partly because of lifestyle changes and better access to diagnosis. The good news is that with timely and adequate medical care, people living with IBD can manage their symptoms and maintain a good quality of life. The more Africans learn about inflammatory bowel disease, the easier it becomes to recognise early signs, seek proper treatment, and reduce the chances of potential complications.
Yes, long-term inflammation from IBD, especially ulcerative colitis, can increase the risk of colon cancer. Regular check-ups and colon screenings help detect changes early.
Yes, children can develop IBD, though it is less common.
1. McDowell C, Farooq U, Haseeb M. Inflammatory Bowel Disease [Updated 2023 Aug 4]. In StartPearls. [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan– [Accessed October 18, 2025]. Available from here.
2. Diez-Martin E, Hernandez-Suarez L, Muñoz-Villafranca C, Martin-Souto L, Astigarraga E, Ramirez-Garcia A, et al. Inflammatory bowel disease: a comprehensive analysis of molecular bases, predictive biomarkers, diagnostic methods, and therapeutic options. Int J Mol Sci. 2024;25(13):7062. doi:10.3390/ijms25137062. Available from here.
3. Watermeyer G, Katsidzira L, Setshedi M, Devani S, Mudombi W, Kassianides C. Inflammatory bowel disease in sub-Saharan Africa: epidemiology, risk factors, and challenges in diagnosis. Lancet Gastroenterol Hepatol. 2022;7(10):952–61. doi:10.1016/S2468-1253(22)00047-4. Available from here.
4. Oshi MA. Inflammatory bowel disease in Africa: the current landscape of pharmacological treatments and the promise of emerging innovations. Explor Drug Sci. 2025;3:1008117. doi:10.37349/eds.2025.1008117. Available from here.
5. Tavakoli P, Vollmer-Conna U, Hadzi-Pavlovic D, Grimm MC. A review of inflammatory bowel disease: a model of microbial, immune and neuropsychological integration. Public Health Rev. 2021;42:1603990. doi:10.3389/phrs.2021.1603990. Available from here.
6. Muzammil MA, Fariha F, Patel T, Sohail R, Kumar M, Khan E, et al. Advancements in inflammatory bowel disease: a narrative review of diagnostics, management, epidemiology, prevalence, patient outcomes, quality of life, and clinical presentation. Cureus. 2023;15(6):e41120. doi:10.7759/cureus.41120. Available from here.
7. Cai Z, Wang S, Li J. Treatment of inflammatory bowel disease: a comprehensive review. Front Med. 2021;8:765474. doi:10.3389/fmed.2021.765474. Available from here.
8. Sasson AN, Ananthakrishnan AN, Raman M. Diet in treatment of inflammatory bowel diseases. Clin Gastroenterol Hepatol. 2021;19(3). doi:10.1016/j.cgh.2019.11.054. Available from here.
Related:
Autoimmune Disorders Simplified for Africans
Colon cancer: Symptoms, Causes, Risk factors
Healthy African Foods for People with Autoimmune Disorders (Misdirected defense)
Understanding Rheumatoid Arthritis: A Guide for Africans
Understanding Rheumatoid Arthritis: Symptoms and Treatment
Published: December 4, 2025
© 2025. Datelinehealth Africa Inc. All rights reserved.
Permission is given to copy, use and share content freely for non-commercial purposes without alteration or modification and subject to source attribution.
DATELINEHEALTH AFRICA INC., is a digital publisher for informational and educational purposes and does not offer personal medical care and advice. If you have a medical problem needing routine or emergency attention, call your doctor or local emergency services immediately, or visit the nearest emergency room or the nearest hospital. You should consult your professional healthcare provider before starting any nutrition, diet, exercise, fitness, medical or wellness program mentioned or referenced in the DatelinehealthAfrica website. Click here for more disclaimer notice.


