Undescended Testicles in African Babies: A Parent’s Practical Guide
By: Kelechi Nwaowu, BNSc, RN. Freelance Medical & Health Writer. Medically reviewed By: Chiamaka Wisdom-Asotah, MB.BS.
July 8, 2026.

An African mother gently bathing her newborn baby boy in a baby tub at home. Image credit. Gemini .
Introduction
When a baby boy is born, one of the first things healthcare workers check is whether both testicles are present and properly positioned in the scrotum. In most babies, the testicles are exactly where they should be. But for some boys, one or both testicles may not be present in the scrotum. This is because the testicles start to develop in the lower belly and gradually find their way out of the belly into the scrotum before birth. When something goes wrong with this process, the condition is called cryptorchidism or undescended testicles in simple words.
For many parents who receive this news, the first reaction is worry, followed by questions like:
These are completely understandable concerns, and this article is here to answer every one of them.
The reassuring truth is that undescended testicles are one of the most common and most treatable conditions in newborn boys. When identified early and managed correctly, most boys grow up to live healthy lives with good fertility outcomes. However, timing matters a lot. The sooner this condition is addressed, the better the long-term results for your son.
Before you can understand why undescended testicles matter, it helps to understand how the testicles develop in a normal pregnancy. This section explains the normal journey that testicles take before birth, and what it looks like when that journey is incomplete.
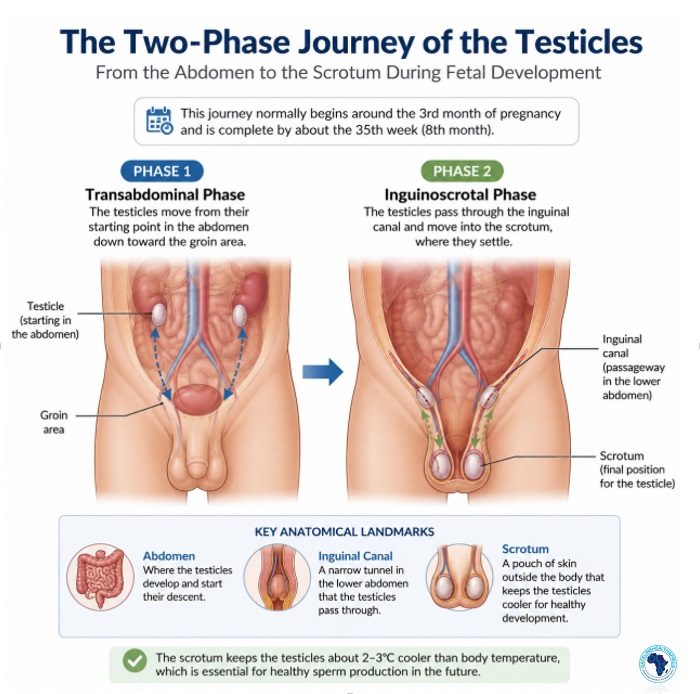
An anatomical image showing the two-phase journey of the testicles from the abdomen to the scrotum. Fact-checked for medical accuracy. ChatGPT. Click on image to enlarge
The testicles are the two small organs found in the scrotum that are responsible for producing sperm and the male sex hormone called testosterone. During pregnancy, a baby boy's testicles do not form in the scrotum. Instead, they develop inside the baby's lower abdomen (lower belly area) (1).
From around the third month of pregnancy, the testicles begin a two-phase journey downward. First, they move from the abdomen toward the groin area. Then, in the second phase, they pass through a narrow passage called the inguinal canal (a small tunnel in the lower belly area) and settle into the scrotum. This entire journey is normally complete by the 35th week (early 9th month) of pregnancy (1).
The scrotum is positioned outside the body, and it helps to keep the testicles about 2 to 3 degrees cooler than normal body temperature. This cooler temperature is important for healthy development and future sperm production (2). This means that for the testicles to produce sperm later as they should, they must be within the cooler environment of the scrotum. And for this to happen, the testicles, which are originally formed in the belly area, must come down to stay inside the scrotum
In some baby boys, one or both testicles do not complete this downward journey as they should. Instead of arriving in the scrotum, they remain somewhere along the way, either inside the abdomen or somewhere within the inguinal canal in the groin area.
When this happens, the condition is called cryptorchidism, which comes from two Greek words meaning "hidden testicle” (1). Note that the testicle is not absent; it is simply not where it should be. And because it is in the wrong place, it is exposed to higher temperatures inside the body, which, over time, can damage the sperm-producing cells.
How Common Are Undescended Testicles?
Cryptorchidism is not a rare condition. In fact, it is the most common genital condition identified in male newborn babies (2). Let's look at the numbers and identify which babies are at greatest risk.
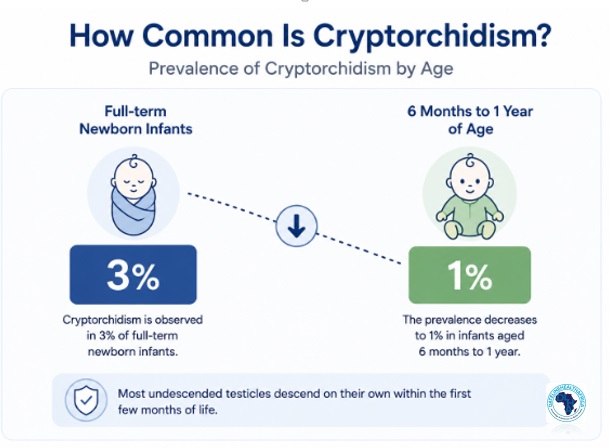
Infographic showing the prevalence of undescended testicles from birth to age one. Illustration created by ChatGPT using prevalence data adapted from StatPearls: Cryptorchidism. Click on image to enlarge.
Globally, approximately 3 in every 100 full-term baby boys are born with at least one undescended testicle (2). In premature babies (those born before 37 weeks of pregnancy), the number rises to approximately 30 in every 100 baby boys born (2). Premature baby boys tend to have the condition more because some are born before the testicles complete their journey to the scrotum.
Despite how common cryptorchidism is, the good news is that most cases resolve without any medical treatment. Around 80% of undescended testicles move into the correct position on their own during the first 3 months of life, as a natural surge of hormones after birth encourages the final descent (1). After this point, however, the testicle rarely descends on its own. This means that by the time a baby reaches 1 year of age, the true occurrence of cryptorchidism reduces to about 1% (2).
Although studies from Africa are limited, available evidence suggests that delayed diagnosis and treatment of undescended testicles remain common in some settings.
A five-year study from the Democratic Republic of Congo found that many boys presented late for care (3). This could mean that many boys born in Africa are not diagnosed and treated when they should, partly because awareness of the condition among parents and community health workers remains low.
Certain factors increase the likelihood of a baby being born with undescended testicles.
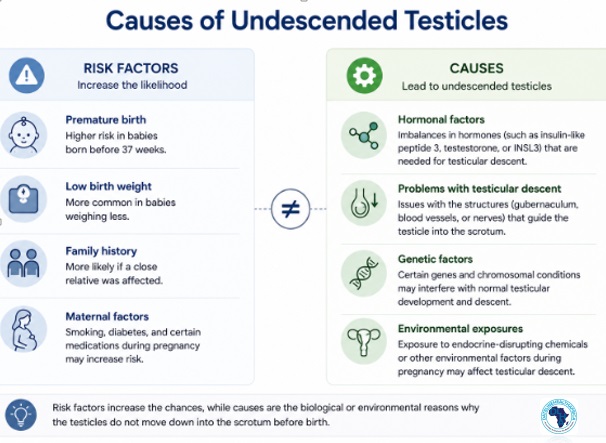
Infographic showing the causes and risk factors of undescended testicles. Click on image to enlarge.
Undescended testicles do not usually have a single, identifiable cause. In most cases, a combination of factors during pregnancy disrupts the processes that guide the testicle into the scrotum. Understanding these factors will help parents and healthcare workers to recognise preventable risks and identify babies who need closer monitoring.
The three main factors linked to undescended testicles are the following:
The downward movement of the testicles is guided by hormones produced by the baby's body, especially testosterone and other growth signals (4).
If the production of these hormones is insufficient, or if their signals are blocked or weakened, the testicle may not receive the chemical instructions it needs to complete its journey. This type of hormonal disruption is the most commonly identified cause of undescended testicles and is responsible for the majority of cases where no other obvious explanation is found (4).
In some boys, undescended testicles occur as a result of a broader genetic condition like Prader-Willi syndrome, Down syndrome, and Noonan syndrome, which are associated with a higher risk of cryptorchidism (2).
A family history of undescended testicles is also a risk factor. If the baby's father, older brother, or other close male relative had the condition, the risk to a new baby boy is higher than in the general population (2). In these cases, extra attention should be paid to checking the baby's scrotal position at birth and during early postnatal visits.
Beyond hormones and genetics, a growing body of research points to the role of the pregnancy environment in testicular descent. Maternal smoking during pregnancy is one of the most consistently documented risk factors, as smoking disrupts the hormonal signals that guide the testicles (1).
Exposure to chemical substances that interfere with the body's natural hormones is another significant concern. These substances are found in:
Pregnant women may be exposed to these chemicals without realising the potential impact they can have on a developing baby. Therefore, avoiding unnecessary chemical exposure during pregnancy, especially in the first and second trimesters, is a simple way to keep your developing baby safe.
One of the most practical things about cryptorchidism is that you, as a parent, can often detect it yourself. This section teaches you exactly what to look for and helps you to understand the difference between one-sided and two-sided undescended testicles.
The simplest and most accessible way to check your baby boy's testicles is during a diaper change or bath time. With clean, warm hands, gently feel the scrotum (the soft skin pouch below the penis). In most cases, you should be able to feel two small, firm, round lumps inside the scrotum. These are the testicles.
If one side of the scrotum feels flat or empty, or if the scrotum as a whole looks unusually small or flat, this may indicate that one or both testicles have not yet descended. It is important to do this check when the baby is warm and relaxed, as cold temperatures cause the scrotum to tighten and draw the testicles upward temporarily – a completely normal occurrence called the cremasteric reflex.
If you notice anything unusual, the right step is to mention it to your doctor or nurse at the next visit. You do not need to panic, but you should not ignore it either.
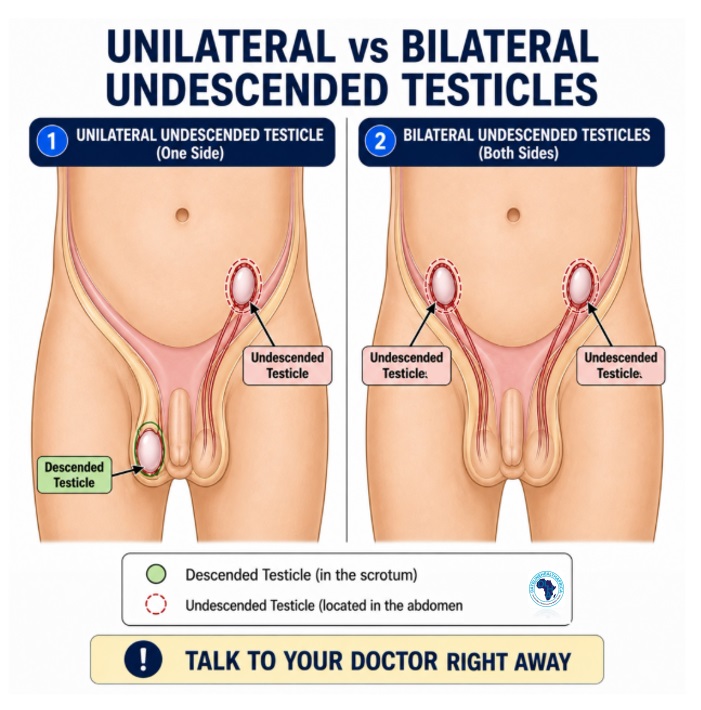
Comparison diagram showing unilateral undescended testicle versus bilateral undescended testicles. Fact checked for medical accuracy. ChatGPT. Click on iamge to enlarge.
Undescended testicles can affect one testicle only, which is called unilateral cryptorchidism, or both testicles, which is called bilateral cryptorchidism.
Unilateral cryptorchidism (affecting only one side) is by far the more common condition, accounting for approximately 90% of all cases, with the right testicle more often affected than the left (2). Boys with unilateral undescended testicles generally have better fertility outcomes than those with bilateral cases, because the other descended testicle continues to develop healthily.
Bilateral cryptorchidism (where neither testicle has descended) occurs in approximately 10% of cases and carries significantly greater risks of infertility if left untreated (2). If both testicles are undescended and neither can be felt by hand during examination, this also raises the possibility of a hormonal or genetic condition that requires further evaluation by a specialist.
Most of the time, the diagnosis of undescended testicles does not require advanced tests. An examination by a skilled nurse or doctor is usually enough to determine whether the testicles are in the scrotum. However, in some cases, additional investigations are needed.
The main method of diagnosing undescended testicles is through physical examination. A trained clinician uses gentle hand pressure to feel the scrotum and groin area. During the examination, the doctor checks whether the testicle can be felt and where it may be located (5).
Routine checks for the position of the testicles should occur at every postnatal visit during the first six months of life. In many African countries, this check should also be a standard part of postnatal care by community nurses and traditional birth attendants, as they are often the first healthcare contact for newborn boys in rural settings.
It is reasonable for parents to wonder whether a scan or imaging test is needed to locate the undescended testicle. However, current international guidelines from multiple organisations state clearly that routine imaging tests are not recommended for most cases of undescended testicles (2). This is because these scans do not improve the accuracy of the diagnosis, and they do not change the treatment recommendation.
Despite this, imaging may occasionally be used in complex cases, such as when both testicles cannot be felt anywhere, and the doctor needs to confirm whether testicular tissue is present at all (2). However, in most situations, the doctor treating the condition will proceed based on the clinical examination alone.
Many parents wonder whether an undescended testicle can simply be left alone. The answer is usually no. Without treatment, the condition can affect fertility and increase the risk of other complications later in life.
The scrotum keeps the testicles cooler than the rest of the body because the sperm cells are highly sensitive to heat. A normal body temperature of around 37°C is too warm for healthy sperm production. The scrotum, on the other hand, maintains a temperature of approximately 33 to 34°C, which is the ideal environment for sperm production (6).
When a testicle remains inside the body, as seen in cryptorchidism, it is exposed to the full 37°C of body heat. Over time, this heat damages the special cells responsible for producing sperm. Research has shown that this damage begins as early as 4 months of age (6).
This has a significant impact on fertility as men with a history of one-sided undescended testicles have an infertility rate of 10% to 30% (2). For men with two-sided undescended testicles, the infertility rate rises to 35% to 65% or higher, and if the condition goes untreated into adulthood, the infertility rate can exceed 90% (2).
To understand other causes of male infertility beyond cryptorchidism, see: Male Infertility in Nigeria: Causes, Symptoms, Diagnosis and Treatment.
An undescended testicle also carries an increased risk of testicular cancer later in life. Men who have an undescended testicle are 3 to 6 times more likely to develop testicular cancer compared to men who do not have the condition (2). Approximately 10% of adults diagnosed with testicular cancer have a history of cryptorchidism (4).
It is important to understand that the corrective surgery for undescended testicles does not fully eliminate this cancer risk. However, it does two important things: it reduces the risk compared to leaving the testicle untreated, and it repositions the testicle into the scrotum, where it can be easily felt and monitored through regular testicular self-examination (2). A testicle hidden like in cryptorchidism cannot be checked for changes, which means any early warning signs of cancer would go unnoticed.
For guidance on how to perform testicular self-examination, see: Testicular Cancer Awareness and Self-Examination Techniques for Africans
An undescended testicle is also more vulnerable to two additional complications, namely: testicular torsion and inguinal hernia (2).
Testicular torsion is a serious condition in which the testicle twists around the cord of blood vessels that supply it. This twisting cuts off the blood supply and, if not treated within a few hours, can permanently damage or destroy the testicle. An undescended testicle is more prone to torsion than a normally positioned one because it is in the wrong location and it has a looser attachment to surrounding tissue (7)
An inguinal hernia, on the other hand, is a condition in which a small section of the intestine or belly tissue pushes through a weak point in the lower belly area near the groin. This condition commonly occurs alongside an undescended testicle and may sometimes be noticed as a soft bulge in the baby's groin area. Both conditions may require surgical correction (8).
For a detailed explanation, see: Testicular Torsion in African Boys: Triggers and Treatment
Beyond the physical complications, boys with undescended testicles may experience emotional and social challenges as they grow older (2). As children become more aware of their bodies, particularly during school-age years and puberty, visible differences from undescended testicles (cryptorchidism) can lead to embarrassment, self-consciousness, and low self-esteem.
While this concern should not outweigh the medical reasons for early treatment, it is an effect that deserves acknowledgement. Early treatment greatly reduces the likelihood of these experiences by correcting the problem before the child is old enough to notice it.
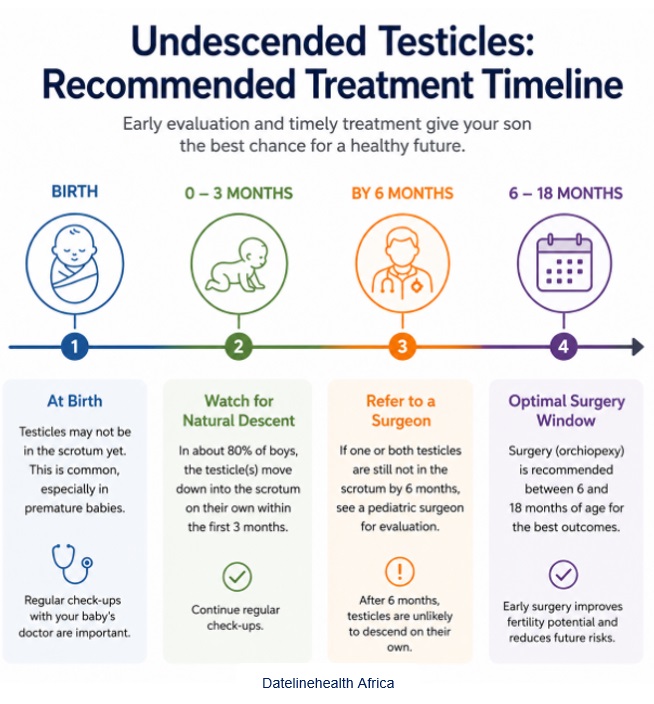
Infographic showing the recommended treatment timeline for undescended testicles from birth to 18 months of age. Click on image to enlatge.
The fact that treatment options exist and work well when used at the right time is genuinely encouraging. Here are the three available approaches to managing undescended testicles:
1. Watchful Waiting
As mentioned earlier, approximately 80% of undescended testicles descend on their own within the first 3 months of life (1). Because of this, doctors do not immediately recommend intervention when the condition is identified at birth. Instead, they advise careful monitoring, especially at each postnatal visit, to note when the testicle has moved into the correct position.
If the testicle has not descended by 6 months of age, then spontaneous descent becomes very unlikely (5). At this point, a discussion with a paediatric (child) surgeon for assessment and planning of further treatment is needed.
Some doctors and clinics use hormonal injections to try to stimulate the testicle to descend (5). These hormones temporarily boost testosterone levels, which may encourage descent in some cases.
However, current international guidelines do not recommend routine hormonal treatment for undescended testicles, because the available evidence shows inconsistent and generally low success rates (2, 5). In practice, hormonal therapy may be considered on an individual basis in certain clinical situations, but it is not a replacement for surgery in confirmed cases. Parents who are offered hormonal treatment should feel comfortable asking their doctor why it is being recommended over surgery and what the expected success rate is.
Orchiopexy or Orchiodoplexy are different names for the surgical procedure used to correct undescended testicles. In this operation, a paediatric (children's) surgeon carefully moves the testicle from its abnormal location (whether in the groin or abdomen) and places it in its correct position inside the scrotum, where it is then stitched lightly in place. The operation is performed under general anaesthesia (a healthcare provider induced state of temporary unconsciousness) and typically lasts for 45 minutes (9).
Orchiopexy is widely regarded as the most effective treatment for undescended testicles and is recommended by virtually all international guidelines (2, 5).
The timing of orchiopexy is one of the most important factors in determining how well a boy's fertility is protected.
Multiple international guidelines recommend that orchiopexy be performed between 6 and 18 months of age (2, 5). This recommendation is strongly supported by research on how the developing testicle changes over time.
A 2017 study of 134 boys with unilateral cryptorchidism found that those who underwent orchiopexy before the age of one year showed significantly better testicular growth than those who had surgery between one and two years, or after two years of age (10). This is because the number of healthy cells within the undescended testicle begins to decline from 4 to 12 months of age, meaning that every month of delay after this point allows further damage (6).
Although boys who have surgery before 1 year of age have better outcomes than those who wait, also noted that boys who receive treatment later still have better outcomes than boys who never receive treatment (2, 10). Therefore, the central message is that early correction leads to better results.
Orchiopexy is a short surgical procedure, and most children recover from it quickly. The majority of boys go home on the same day of the operation (11). The attending surgeon will provide specific instructions about wound care, pain management, and activity restrictions.
After surgery, it is normal for the treated area to be slightly swollen and tender for a few days. However, most children return to normal activity within two weeks (11). Parents should watch for signs of infection, such as increasing redness, warmth, or discharge at the wound site, and should contact the surgeon if these signs appear.
Regular follow-up appointments are an important part of care after orchiopexy. At these visits, the surgeon confirms that the testicle has remained in its correct position and is developing as expected. Long-term monitoring is also important because of the slightly increased risk of testicular cancer in men who have had cryptorchidism (2).
In terms of fertility, the outlook for boys who are treated is encouraging. For example, 70-90% of boys who were treated for unilateral undescended testicles have approximately normal ability to father children (2).
Boys with bilateral undescended testicles who receive early surgical treatment have lower chances than those with unilateral cryptorchidism; however, they are still significantly better than those who receive treatment late or not at all (2). It is also reassuring to know that recurrence after surgery is uncommon. After a successful orchidopexy, only about 1-5% of treated boys experience the testicle moving back into the belly area (2)
Note that as your son reaches his teenage years, it is important to teach him to perform regular self-examinations of the testicles. This practice takes only a few minutes and allows early detection of any changes that may indicate cancer or other conditions.
Undescended testicle(s) is a common condition, and for the many parents who receive this diagnosis about their son, the most important message to take away here is this: early action makes all the difference.
When treatment, particularly orchiopexy, is performed between 6 and 18 months of age, most boys go on to live healthy lives with normal or near-normal fertility outcomes. The risks associated with leaving the condition untreated include infertility, testicular torsion, and cancer. Although they are real, they are also largely preventable.
As a parent, you have a powerful role to play. Check your baby boy's scrotum during bath time and diaper changes in the first weeks of life. If you feel that one side seems flat or empty, mention it to your healthcare provider without delay. Attend all postnatal and well-child appointments. And if your son is diagnosed with undescended testicles, follow through with the recommended treatment and follow-up appointments.
Your early action is the foundation of your son's future health.
Yes. In many baby boys, the testicle moves into the scrotum on its own within the first few months after birth. If it has not descended by six months of age, it is less likely to correct itself and should be checked by a doctor.
Experts recommend surgery between 6 and 18 months of age, with many guidelines preferring treatment before the child's first birthday. Early treatment helps protect fertility and reduces the risk of future complications.
Many boys treated early for an undescended testicle grow up to have normal fertility. However, delayed treatment can affect sperm production and reduce fertility later in life, especially if both testicles are affected.
Most babies and children with an undescended testicle do not feel pain. The condition is often noticed because one or both testicles cannot be felt in the scrotum. Pain in the scrotal area should always be reported to a doctor, as it may signal another problem.
1. Holmboe SA, Beck AL, Andersson AM, Main KM, Jørgensen N, Skakkebæk NE, Priskorn L. The epidemiology of cryptorchidism and potential risk factors, including endocrine disrupting chemicals. Frontiers in endocrinology. 2024 Apr 3;15:1343887. Available from here.
2. Leslie SW, Sajjad H, Villanueva CA. Cryptorchidism. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 May 5 [cited 2026 Jun 24]. Available from here.
3. Désiré AM, Buhendwa C, Césaire TM, Prisca KI, Levi LN, David NB, Longombe AO, Pierre W. Epidemiology, diagnosis and therapeutic approaches of cryptorchidism at the Panzi General Hospital, DR Congo: A 5-year retrospective study. Ethiopian Journal of Health Sciences. 2020 Jan;30(1):107. Available from here.
4. Abaci A, Çatli G, Anik A, Böber E. Epidemiology, classification and management of undescended testes: does medication have value in its treatment?. Journal of clinical research in pediatric endocrinology. 2013 May 30;5(2):65. Available from here.
5. Shin J, Jeon GW. Comparison of diagnostic and treatment guidelines for undescended testis. Clinical and experimental pediatrics. 2020 Mar 23;63(11):415. Available from here.
6. Wang X, Liu Q, Zhuang Z, Cheng J, Zhang W, Jiang Q, Guo Y, Li R, Lu X, Cui L, Weng J. Decoding the pathogenesis of spermatogenic failure in cryptorchidism through single-cell transcriptomic profiling. Cell Reports Medicine. 2024 Sep 17;5(9). Available from here.
7. Baldanza F, Grasso F, Sergio M, Patti M, Maggiore V, Serra G, Giuffré M, Corsello G, Di Pace MR, Pensabene M. Testicular Torsion in Inguinal Cryptorchidism: Report on Two Patients and Literature Review. Children. 2025 Nov 13;12(11):1531. Available from here.
8. Kimura D, Miyagawa Y, Miyao M, Matumura H, Koike S. An adult right inguinal hernia and cryptorchidism treated simultaneously with laparoscopic transabdominal preperitoneal repair and laparoscopic orchiectomy: a case report. Journal of Surgical Case Reports. 2024 Feb;2024(2):rjae096. Available from here.
9. UPMC Children's Hospital of Pittsburgh. Undescended testicle (orchiopexy) repair surgery [Internet]. Pittsburgh (PA): UPMC Children's Hospital of Pittsburgh; [cited 2026 Jun 24]. Available from here.
10. Tseng CS, Chiang IN, Hong CH, Lu YC, Hong JH, Chang HC, Huang KH, Pu YS. Advantage of early orchiopexy for undescended testis: Analysis of testicular growth percentage ratio in patients with unilateral undescended testicle. Scientific Reports. 2017 Dec 12;7(1):17476. Available from here.
11. Children's Hospital Colorado. Orchiopexy [Internet]. Aurora, CO: Children's Hospital Colorado; 2026 [cited 2026 Jun 24]. Available from here.
Published: July 8, 2026
© 2026. Datelinehealth Africa Inc. All rights reserved.
Permission is given to copy, use, and share content freely for non-commercial purposes without alteration or modification, and subject to attribution as to source.
DATELINEHEALTH AFRICA INC., is a digital publisher for informational and educational purposes and does not offer personal medical care and advice. If you have a medical problem needing routine or emergency attention, call your doctor or local emergency services immediately, or visit the nearest emergency room or the nearest hospital. You should consult your professional healthcare provider before starting any nutrition, diet, exercise, fitness, medical or wellness program mentioned or referenced in the DatelinehealthAfrica website. Click here for more disclaimer notice.


