Tech Age Woes: How Digital Health Misinformation Costs African Lives
By Mosope Ososanya. Freelance Health Writer. Reviewed by: Adebowale Bello. B.Tech Microbiology. DLHA Fellow.
June 4, 2026

Description: Illustration of people in Africa using smartphones as health misinformation spreads through social media and digital networks across the continent. Image Credit: ChatGPT-4. Click on image to enlarge.
There is no doubt that technology is taking over several sectors across the world, and Africa is no exception.
In many African countries, this rapid digital shift is being driven by the widespread adoption of smartphones and increasing internet access.
It is estimated that around 74% of people who access the internet in Africa are connected via mobile phones, making smartphones the dominant gateway to digital information in Africa (1).
The increasing smartphone adoption and internet access are also reshaping the healthcare system in Africa in ways that include telemedicine platforms, AI-assisted diagnostics and mobile health applications for maternal and chronic disease management (2).
However, smartphones, which are the primary gateway to health information for most Africans, are also the main tool for propagating health misinformation.
The World Economic Forum has identified misinformation and the technology that amplifies it as one of the top global risks facing humanity today (3). Health misinformation should be treated as a serious public health threat (4).
This article examines the role of technology in spreading health misinformation in Africa, the extent to which health misinformation threatens public health, types of health misinformation and how all stakeholders affected by misinformation can work together to fight the spread of health misinformation on the continent.
Info-poster showing an African physician defining health misinformation in a callout box. Created through prompts in ChatGPT. Click on image to enlarge.
Health misinformation refers to any false or misleading health-related claim that is not grounded in valid evidence or scientific knowledge. It is not always deliberate. It is also different from disinformation.
Misinformation is the spread of false information without the intent to mislead. Those who share it may genuinely believe it to be true, useful, or interesting. Disinformation, on the other hand, is false information spread with full knowledge of its inaccuracy, and with deliberate intent to deceive.
For example, your neighbour sharing an herbal remedy “cure” for diabetes on a WhatsApp group is spreading misinformation, but the company selling that same remedy with fabricated clinical trial data is engaging in health disinformation.
Related: Caution: Health misinformation abound on the internet
Health misinformation is not just harmless rumours. People make important health decisions based on what they know about a health problem: How serious it is, how likely they are to be affected, and whether recommended treatments are safe and effective. When that knowledge is built on false information, the decisions that follow can cause serious harm.
During the COVID-19 pandemic, health misinformation led people to decline vaccines, reject public health measures, and use unproven treatments (5).
Health misinformation also erodes the public’s trust towards the healthcare system, and this makes people more susceptible to further misinformation. In many communities across Africa, where trust in public health institutions is already weak, this cycle needs to be stopped.
Misinformation affects vulnerable communities more, making existing health challenges worse. It affects rural communities, low-income populations, and people with limited access to reliable health information the most, the same groups that public health programmes are working hardest to reach.
Related: Misinformation and Disinformation in the era of Covid-19 are no exception
Info-poster showing several ways in which technology is used to amplify health misinformation. Created through prompts in ChatGPT. Click on image to enlarge.
Social media platforms have changed how information travels, and not always for the better. Facebook, X (Formerly Twitter), TikTok, YouTube, and Instagram give any user the ability to publish and broadcast health claims instantly, without editorial or scientific review.
Social media algorithms are designed to prioritise content that evokes reactions regardless of accuracy. Many so-called health and wellness influencers, brands, and blogs take advantage of this, using clickbait to spread misinformation for the purpose of popularity on social media (6).
In Africa, Facebook remains the dominant platform for health information sharing. A structured review of health misinformation on social media in Africa found that Facebook alone accounted for 52.3% of vaccine-related misinformation, outpacing WhatsApp, Twitter, and YouTube combined (7).
Messaging apps are another key tool for spreading health misinformation. WhatsApp is the most widely used communication platform in Kenya, South Africa, and Nigeria, with monthly active users aged 16–64 reaching 97%, 96%, and 96% respectively (8). It is fast, accessible, and costs very little data, making it ideal for mass communication.
However, the closed nature of WhatsApp and other messaging platforms makes monitoring nearly impossible. The end-to-end encryption feature within WhatsApp allows users to share messages without monitoring from the WhatsApp team, which makes it an unsupervised platform (8).
When a false health claim is shared by a friend, family member, or trusted community figure, most people do not stop to verify it, because the trust they have in the person overrides the need to question the information. The message is endorsed, and so it is believed, acted upon, and forwarded to the next person, who trusts the sender just as much.
A newer but rapidly growing threat is the use of artificial intelligence to generate and amplify health misinformation.
The emergence of generative AI tools, like image and video generators, voice cloning, and AI animated graphics, has increased both the quantity and spread of health misinformation (9).
AI-generated deep fakes are designed to make false health claims appear credible. Healthcare practitioners and organisations are raising serious concerns about how real this generative AI content looks, particularly deep fake videos depicting trusted medical experts sharing misleading health information (10).
In a study, fact-checkers uncovered hundreds of manipulated videos using altered footage of respected health experts to promote unregulated supplements targeting health topics like menopause, hypertension and arthritis (11).
Research has shown that AI-generated misinformation is often more challenging for both humans and automated detectors to identify, and its deceptive style can cause harm (9). For many African users who are less familiar with digital technology, this threat is even greater.
Search engines are built to serve users what they are most likely to engage with and not necessarily what is most accurate.
Content recommendation systems also work in ways that may promote health misinformation. When someone searches for information about a health condition and clicks or engages with misinformed result, the algorithm learns from that behaviour and serves more of the same, a cycle that gets worse over time.
This is the foundation of what researchers call the “echo chamber” effect. Short-video platforms such as TikTok often trap users in repetitive content loops created by engagement algorithms (12), meaning someone exposed to false claims about herbal cures for diabetes may never encounter a correction, because the algorithm never shows them one.
For communities where search engines and social platforms may be the primary source of health information, the consequences of algorithm and search engine recommendations are significant
The internet has made it possible for everyone to create and share content, not just professionals. Influencers, bloggers, online activists, and everyday people with smartphones are now creating and sharing news, making information more accessible to everyone.
The problem with everyone publishing freely is that there’s very little control over what gets shared and because social media and messaging apps make it very easy to share content, false information also spreads quickly (13)
A UNESCO survey found that 63% of influencers lack rigorous fact-checking protocols, despite their significant impact on public discourse (14). In Kenya and Nigeria, a 2023 report found that 94.87% of surveyed participants actively follow social media influencers (15).
False medical cures, unregulated supplement endorsements, and anti-vaccination rumours spread fastest through these channels, often framed as personal testimonials or community wisdom. Africa Check, one of Africa’s leading fact-checking organisations, has consistently documented health misinformation as one of the most prevalent categories it verifies (16).
Understanding why health misinformation spreads so easily in Africa is also important.
The ability to evaluate online health information is not just about having internet access. It requires specific skills and exposure that many people in Africa are still developing. Research suggests that those with low digital health literacy are significantly more likely to seek health information from unreliable sources (17).
A systematic review found that low digital literacy is one of the main barriers to finding health information online in African countries. It also found that many people struggle to judge whether online sources are trustworthy (18).
This challenge affects more than just everyday users or people with low literacy levels. Another systematic review and meta-analysis of digital literacy among health professionals in Ethiopia found that the overall digital literacy level was relatively low. The study also showed the need for focused efforts, such as computer training and education programmes, to help people improve their digital literacy skills (19).
When health professionals themselves struggle to navigate digital information environments, the challenge for the general population is even greater. Without the ability to distinguish a peer-reviewed study from a viral Facebook post, or a registered healthcare provider from an anonymous account claiming medical expertise, users are at risk of health misinformation.
In Africa, health decisions are rarely a “one man” decision. Family, community, religious leaders, and peers play a powerful role in shaping what people believe about their health.
This is not totally a problem; community trust networks are also important for spreading accurate health information. The problem is when those networks carry misinformation.
Research on how health information is shared in communities show that trust and strong relationships help people learn and accept health messages. However, rumours passed through friends and community networks, such as claims that blood sample collection is a malign government agenda, can make people less likely to take part in health programmes (20).
COVID-19 vaccine hesitancy was driven by false claims that gained credibility not because of its evidence base, but because of who was sharing it. When a respected pastor, community elder, or trusted family member openly declares their belief on a health subject, it is perceived as legitimate immediately.
More than 2,000 languages are spoken across Africa, but most reliable online health information is only available in English, French, or Portuguese. This lack of health content in local languages is a major barrier to accessing trustworthy health information online in many African countries (21).
When people cannot find accurate health information in a language they understand, they rely on whatever is available. And people often spread misinformation in local languages, dialects, and familiar cultural style because that is where people are more likely to trust it.
Language barriers in healthcare can lead to avoidable medical mistakes, poor adherence to treatment, reduced use of health services, and lower satisfaction with formal healthcare systems (22).
When digital health information is also hard to understand, because it uses complex language or ignores local languages entirely, people are more likely to turn to simpler health claims shared in languages they understand, like urban and broad Pidgin, Hausa, Yoruba, or Amharic, even when those claims are not accurate.
One of the major drivers of health misinformation in Africa is lack of access to healthcare. Millions of people do not have easy access to professional healthcare. Africa has a physician density of just 2.9 doctors per 10,000 people, far below the WHO-recommended minimum of 44.5 health workers per 10,000 (23).
Long distances to the nearest clinic, unaffordable consultation fees, long waiting times, and traditional beliefs are all barriers to formal care. This alone makes many Africans turn to the internet, including social media and AI chatbots as a first resort.
In addition, there is a shortage of trusted, verified health information from official institutions in African contexts (24). When credible, culturally relevant, locally accessible health information is scarce, misinformation does not struggle to find an audience.
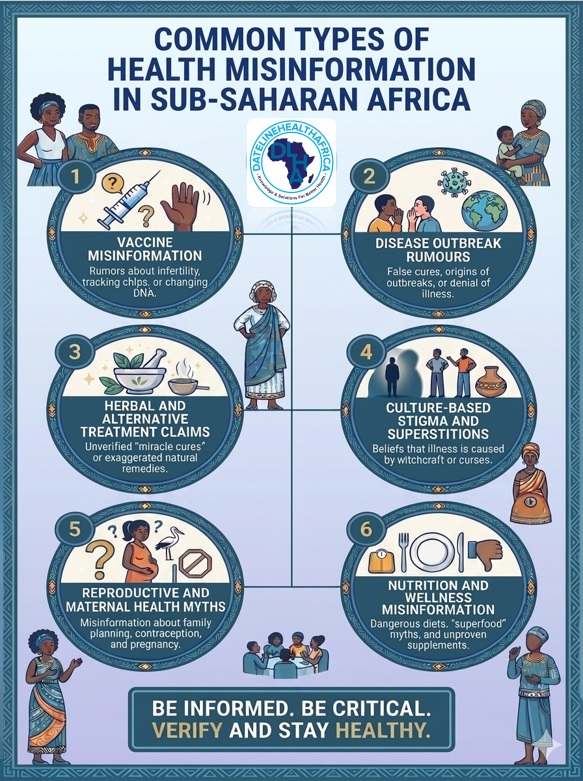
An info-poster illustrating examples of common types of health misinformation in sub-Saharan Africa. Created through prompts in Nano Banana 2. Click on image to enlarge.
Health misinformation may come in different forms. A few include:
This is the most dangerous and well-documented category. Claims that vaccines cause infertility, contain microchips, or are tools of Western population control have circulated for years across social media and WhatsApp groups.
In 2024, a single ten-minute video by a Kenyan anti-vaccine advocate, spreading false claims about tetanus, malaria, and HPV vaccines, gained over 938,000 views on X and was widely shared on WhatsApp across Nigeria, Kenya, Uganda, Ethiopia, and the Democratic Republic of Congo (25).
In South Africa, AIDS denialism, which is the false belief that HIV does not cause AIDS, was adopted at the highest levels of national government, reducing access to effective treatment and contributing to over 330,000 preventable deaths (26).
During the Marburg virus scare in Africa, false health claims caused a 70% surge in WhatsApp chain messages, triggering panic-buying of food and medical supplies across communities (27). During Ebola outbreaks, rumours that healthcare workers were harvesting organs or that treatment was dangerous led many people to hide those who were sick and stay away from healthcare facilities, which worsened transmission and outcomes.
These are deeply rooted in the African health information landscape. WHO’s Africa Infodemic Response Alliance reported a sharp increase in social media posts promoting unproven herbal treatments for malaria and measles. It warned that these claims could make both diseases more dangerous by discouraging people from seeking proper medical care (28).
The reason herbal and alternative treatment claims thrive in Africa is that traditional medicine is culturally familiar, affordable, and accessible. The problem comes when people accept these remedies as total substitutes for evidence based medical treatments.
Rumors or health misinformation claiming that certain illnesses, or conditions are caused by witchcraft or malicious individuals have often incited deadly mob violence against health workers and community members. Also, such culture-based misinformation has for example contributed to neglect and withholding of emergency care and support for individuals having epilepsy.
This category of health misinformation remains stubbornly persistent, circulating through both digital and traditional channels. False claims about contraceptives causing permanent infertility, unsafe home delivery practices endorsed online, and misinformation about breastfeeding and newborn care continue to undermine maternal and child health outcomes, particularly in communities where formal antenatal education is limited or distrusted.
Affordability makes the problem even worse. In many African countries, some pregnant women avoid hospitals and instead go to traditional birth attendants or “massage homes” because hospital delivery is too expensive. When misinformation online also supports this choice by suggesting that hospital births are unsafe, unnecessary, or not culturally appropriate, it becomes even harder for public health programmes to encourage hospital deliveries, antenatal, and postnatal care.
Viral claims about miracle foods that cure diabetes, cancer, or hypertension are common health content across African social media spaces. During COVID-19, many people started using herbal supplements much more often and this was driven by cultural beliefs, easy access, and the idea that they might work, even though there was no clinical evidence to support their effectiveness (29). Posts promoting extreme dietary restrictions, unregulated supplements, or dangerous detox regimens circulate freely, with no policy to stop them.
Related: How to Spot Health Misinformation and What To Do About It, According To Experts
Health misinformation has numerous consequences for individuals, healthcare systems, and public health in general.
At the individual level, the most immediate consequence is delayed treatment. In Ethiopia, studies have shown that health misinformation has led to delays in treating illnesses like Tuberculosis and HIV, lower use of vaccines and maternal health services, and ongoing stigma around certain diseases (30).
When someone follows online advice to manage a serious illness with herbal remedies instead of seeking clinical care, it results in delays in receiving proper medical care. A study has shown that false information about symptoms and treatments leads people to delay seeking medical help, with serious consequences for outcomes, particularly for diseases where early detection and treatment are decisive (31).
Beyond health, misinformation also costs people money. Unproven supplements, traditional remedies promoted on social media, and fake “cure” packages sold through WhatsApp and Facebook take money from people who least can afford it. In places without health insurance and where people pay directly for most healthcare, these losses make an already difficult situation even worse (32).
Misleading information about diseases, treatments, and vaccines reduces the public’s trust in science and the healthcare system (33).
When patients arrive at clinics having already self-medicated based on viral social media advice, it becomes more complicated and more expensive.
During disease outbreaks, the pressure becomes even greater: health workers have to deal with the disease itself and the misinformation surrounding it, often fighting two epidemics at once. During the Ebola crisis, COVID-19, and various polio campaigns, healthcare workers in Africa faced active community resistance, harassment, and in some cases violence fuelled by false claims, diverting resources and attention from the actual emergency (33).
Vaccine hesitancy driven by misinformation is one of the most damaging public health consequences. As of October 2022, Africa lagged significantly behind the rest of the world with only 24% full COVID-19 vaccination coverage, compared to 63% globally. This is partly a result of the spread of anti-vaccination rumours, as well as structural barriers (34).
The spread of false claims linking COVID-19 vaccines to severe long-term side effects fuelled hesitancy across multiple African countries, with even some healthcare workers reluctant to take the vaccine due to misinformation-induced doubts about its effectiveness (35).
This contributes to the spread of diseases that could otherwise be prevented such as measles outbreaks in communities with low vaccination rates, the return of polio in areas where vaccination campaigns face resistance, and avoidable maternal deaths in communities where misinformation has portrayed hospital delivery as harmful.
Now that we understand the problem of technology-driven health misinformation in Africa, we can look at ways to address it and use technology more effectively.
AI tools are increasingly being used to track how health misinformation spreads in real time. They scan social media posts, flag suspicious health claims, and help fact-checkers detect false information more quickly. In Africa, organisations like Fact Check Africa have already started using AI in their newsroom work.
The potential in using AI to combat health misinformation is significant, but there are limitations, particularly around language diversity and data gaps.
Technology evolves faster than legislation, hence governments cannot afford to stay passive. Several African countries are beginning to develop digital governance frameworks that address online misinformation, some more effectively than others.
Balancing policy regulation is important. Policies that are too strict can limit free expression and lead to censorship, while policies that are too weak allow false and harmful information to spread without control.
Social media platforms that spread health information also have both the responsibility and the ability to reduce misinformation. They can do this through content moderation, working with fact-checkers, and making their algorithms more transparent and accountable.
For example, YouTube now uses a verification label for licensed health professionals, which helps users tell the difference between qualified medical practitioners and general influencers sharing health advice.
Despite this, progress has not been steady. Recent decisions by major platforms, like Meta (Facebook and Instagram) to reduce its reliance on third-party fact-checkers because of a so-called community-driven approach is concerning.
Radio, television, and print media remain among the most trusted information sources across large parts of Africa, particularly in rural areas and among older populations.
Public health campaigns that use these channels and work with community radio stations and local-language print media can reach people and build trust in ways that digital platforms often cannot in many places. However, these approaches can also be limited by factors like funding, reach, and the speed at which information can be shared compared to digital platforms.
Technology helps spread health information in Africa, but it also spreads misinformation at the same time. The same digital systems that are improving healthcare delivery are also carrying harmful false health claims into homes, community groups, and medical decisions every day.
The problem is not the technology itself, but how it is used, who controls it, and whether it prioritises accuracy over attention and engagement.
Reducing health misinformation in Africa requires governments, tech platforms, healthcare communicators, and communities to work together toward the same goal. When false health information is left unchecked, patients are the ones who suffer the most consequences.
1. Tila C. Internet penetration in Africa February 2025, by country.Statistica [Internet]. Nov. 7, 2025. Cited June 20, 2026. Available from here:
2. Benecke RM, Asiimwe IG, Abulfath AA, et al. Digital health innovations in Africa: Harnessing AI, telemedicine, and personalized medicine for improved healthcare. Frontiers in Pharmacology. 2026, Volume 17. Doi: 10.3389/fphar.2026.1799832. Available from here.
3. World Economic Forum. Global risks report 2024. [Internet] 10 January 2024. [Cited June 23, 2026]. Available from here.
4. Kbaier D, Kane A, McJury M, Kenny I. Prevalence of Health Misinformation on Social Media-Challenges and Mitigation Before, During, and Beyond the COVID-19 Pandemic: Scoping Literature Review. Journal of medical Internet research, 2024;26, e38786. Doi: 10.2196/38786. Available from here.
5. U.S. Department of Health and Human Services. Health misinformation: Surgeon General's advisory. [Internet, n.d.]. Cited June 23, 2026. Available from here.
6. Denniss E, Lindberg R. Social media and the spread of misinformation: Infectious and a threat to public health. Health Promotion International, 2025;40(2), daaf023. Available from here.
7. Hove C, Cilliers L. A structured literature review of the health infodemic on social media in Africa. Jamba (Potchefstroom, South Africa), 2023;15(1), 1484. Available from here.
8. Mmadu-Okoli C, Nsofor I. WhatsApp, COVID-19 related misinformation in Africa and the need for continuous infoveillance. HPHR Journal, 2021;39.10.54111/0001/MM8. Available from here.
9. Zhang, Z., Zhang, Y., Zhou, X., Huang, L., Razzak, I., Nakov, P., & Naseem, U. From generation to detection: A multimodal multi-task dataset for benchmarking health misinformation. arXiv preprint arXiv. 2025;2505.18685. Available from here.
10. The Conversation. Generative AI and deep fakes are fuelling health misinformation. [Internet]. March 13, 2025. [Cited June 23, 2026]. Available from here.
11. National Public Health Information Coalition. AI deep fakes of real doctors spreading health misinformation on social media. [Internet]. 22nd December 2025. [Cited June 23, 2026]. Available from here.
12. Hassani Saissi M, Idrissi N, Zellou A. Understanding echo chambers in recommender systems: A systematic review. International Journal of Advanced Computer Science and Applications, 2025;16(10), Article 71. Available from here.
13. Badji SD, Orgeret KS, Mutsvairo B. An Exploratory Study of Fact-Checking Practices in Conflict and Authoritarian Contexts. Media and Communication, 2024;12, Article 8698. Available from here.
14. UN News. United Nations Educational, Scientific and Cultural Organization. 2/3 of digital content creators do not fact-check. [Internet] 27 November 2024. [Cited June 23, 2026]. Available from here.
15. Simba H, & Girma E. Optimizing social media influencers for health communication in Africa. Global health action, 2025;18(1), 2572009. Available from here.
16. Africa Check. From election myths to health misinformation: Top 5 claims fact-checked in 2024. [Internet] 29th December 2024. [Cited June 23, 2026]. Available from here.
17. Yuen E, Winter N, Savira F, Huggins CE, Nguyen L, Cooper P, Peeters A, Anderson K, Bhoyroo R, Crowe S, Ugalde A. Digital health literacy and its association with sociodemographic characteristics, health resource use, and health outcomes: Rapid review. Journal of Medical Internet Research, 2024;13, e46888.Available from here.
18. Chereka AA, Shibabaw AA, Butta FW, Tadesse MN, Abebe MT, Atanie FA, Kitil GW. Explore barriers to using the internet for health information access in African countries: A systematic review. PLOS Digital Health 2025;4(1), e0000719. Available from here.
19. Chereka AA, Walle AD, Kassie SY, Shibabaw AA, Butta FW, Demsash AW, Hunde MK, Dubale AT, et al. Evaluating digital literacy of health professionals in Ethiopian health sectors: A systematic review and meta-analysis. PloS one, 2024;19(5), e0300344. Available from here.
20. Mukoka M, Mhango O, Twabi HH, Chipandwe C, Semphere R, Msosa TC, Nliwasa M, et al. The influence of social networks in adoption of integrated health interventions: A qualitative study of fishermen in Malawi. PLOS global public health,2025;5(6), e0004581. Available from here.
21. Taylor A, Kazembe P. Assessing language barriers in health facilities in Malawi. BMC Health Services Research. 2024;24, 1393. Available from here.
22. Olani AB, Olani AB, Muleta TB, Rikitu DH, Disassa KG. Impacts of language barriers on healthcare access and quality among Afaan Oromoo-speaking patients in Addis Ababa, Ethiopia. BMC Health Services Research, 2023;23, 39. Available from here.
23. World Health Organization. Health workforce. [Internet, n.d.]. Cited June 23, 2026. Available from here.
24. Nigatu HH, Abdelkadir NA, Tewelde F, Chancellor S, Wilkinson D. Into the void: Understanding online health information in low-web data languages. arXiv preprint arXiv:2025;2509.20245. Available from here.
25. World Health Organization Regional Office for Africa. WHO AIRA infodemic trends report: 27 May – 3 June 2024. [Internet, n.d.]. Cited June 23, 2026. Available from here.
26. U.S. Department of Health and Human Services. Confronting health misinformation: U.S. Surgeon General's advisory. [Internet, n.d.]. Cited June 23, 2026. Available from here.
27. SQ Magazine. Social media misinformation statistics 2025. [Internet] June 2025. [Cited June 23, 2026]. Available from here.
28. World Health Organization Regional Office for Africa. WHO AIRA infodemic trends report: 12–19 September 2023. [Internet, n.d.]. Cited June 23, 2026. Available from here.
29. Onyeaghala AA, Anyiam AF, Husaini DC, Chiroma JH, Arinze-Anyiam OC. Exploration of vaccination and herbal supplement usage preferences among African populations during coronavirus disease 2019 pandemic: A scoping review. Journal of Herbal Medicine, 2025;51, 101016. Available from here.
30. Berhe TT, Jara D, Kifle D. Health Misinformation in Ethiopia: Myths, Media Dynamics, Public Response, and Policy Implications: A Narrative Review. Public health challenges, 2025;5(1), e70181. Available from here.
31. Kazemi A, Mihalcea R. Misinformation as information pollution. arXiv preprint arXiv:2306.2023;12466. Available from here.
32. Nicholas A, Deji, O. Invisible illness: The consequences of limited health insurance in Africa. Health science reports, 2023;6(6), e1313. Available from here.
33. World Health Organization. WHO looks back at 2024. [Internet] 24th December 2024. [Cited June 23, 2026]. Available from here.
34. Njoga EO, Awoyomi OJ, Onwumere-Idolor OS, Awoyomi PO, Ugochukwu ICI, Ozioko SN. Persisting Vaccine Hesitancy in Africa: The Whys, Global Public Health Consequences and Ways-Out-COVID-19 Vaccination Acceptance Rates as Case-in-Point. Vaccines, 2022;10(11), 1934. Available from here.
35. Duga A, Njagi D, Nyikuri M, Ojo J, Fallah MP, Raji T. COVID-19 vaccine hesitancy in Africa. [Internet], October 25, 2023 Think Global Health. [Cited June 23, 2026]. Available from here.
Published: June 4, 2026
© 2026. Datelinehealth Africa Inc. All rights reserved.
Permission is given to copy, use and share content for non-commercial purposes without alteration or modification and subject to source attribution.
DATELINEHEALTH AFRICA INC., is a digital publisher for informational and educational purposes and does not offer personal medical care and advice. If you have a medical problem needing routine or emergency attention, call your doctor or local emergency services immediately, or visit the nearest emergency room or the nearest hospital. You should consult your professional healthcare provider before starting any nutrition, diet, exercise, fitness, medical or wellness program mentioned or referenced in the DatelinehealthAfrica website. Click here for more disclaimer notice.


